

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The high mortality and morbidity rates that characterize stroke have made it an important public health problem, not only in Korea but also globally. New-onset or recurrent stroke is diagnosed in ~105,000 patients in Korea every year, and more than 26,000 patients die due to this condition [1]. In fact, after cancer, stroke is the second leading cause of death worldwide, resulting in an annual mortality rate of 53.2 per 100,000 in 2010 [1].
High-sensitivity cardiac troponin T and I (cTnT and cTnI) levels have been well-documented as sensitive and specific biomarkers of myocardial necrosis [2]. Recently, elevated cardiac troponin levels were reported not only in patients with ischemic myocardial damage but also in those with acute ischemic stroke [34]. The causes of elevated cTnT levels and the mechanisms by which cTnT is elevated in patients with acute ischemic stroke are variable and the clinical significance is still unclear [34].
In some studies, an elevated cTnT level was a predictor of poor clinical outcomes and higher mortality in patients with acute ischemic stroke [567]. In contrast, other studies have reported that an elevated cTnT level in patients with acute ischemic stroke was not an independent predictor of the clinical outcome and had no significant association with mortality [8910]. Therefore, the value of the cTnT level as an independent prognostic indicator in patients with acute ischemic stroke is uncertain. Thus, the aim of this study was to investigate the prognostic relevance of cTnT levels in patients with acute ischemic stroke.
MATERIALS AND METHODS
1. Study Population
From January to December 2012, 293 consecutive patients with new-onset acute ischemic stroke admitted to the Stroke Center of Ewha Womans University Mokdong Hospital were screened. Acute ischemic stroke was confirmed by magnetic resonance imaging as well as diffusion-weighted imaging. The exclusion criteria were as follows: patients who visited the emergency room >72 hr after the onset of the symptoms (n=2); patients with cTnT data missing on admission (n=1); patients with atrial fibrillation (n=34), patients with prolonged QT (n=9) and other miscellaneous abnormalities (n=9) observed in electrocardiogram findings; patients with abnormal echocardiogram findings (n=24); patients with a medical history of intracerebral hemorrhage (n=2) or cardiovascular diseases (n=3); and patients who failed to follow-up (n=27). Finally, 182 patients were included in this study. The patient selection process is described in Fig. 1. This study was approved by the Institutional Review Board of Ewha Womans University Mokdong Hospital (approval number: ECT 13-03A-22).
2. Data Collection
Age, sex, clinical characteristics, and comorbidities (hypertension, diabetes mellitus, and dyslipidemia) were retrospectively obtained from the patients' medical records. Electrocardiography and echocardiography results and laboratory test results, including measurements of cTnT, creatine kinase (CK), CK-MB, aspartate transaminase (AST), lactate dehydrogenase (LD), complete blood cell count (CBC), glucose, blood urea nitrogen (BUN), creatinine, triglycerides, cholesterol, albumin, C-reactive protein (CRP), fibrinogen, fibrin degradation product (FDP), D-dimer, low-density lipoprotein (LDL) and high-density lipoprotein (HDL), were also collected. To assess stroke severity and prognosis, the National Institutes of Health Stroke Scale (NIHSS) score on admission, the modified Rankin Scale (mRS) on discharge, and all-cause mortality 30 days after stroke onset were obtained.
3. High-sensitivity cTnT Assay
Serum cTnT concentrations on hospital day 1 were measured using the 4th generation Elecsys Troponin T assay (Roche Diagnostics, Mannheim, Germany) on an Elecsys 2010 analyzer (Roche Diagnostics) [11]. The limit of detection and the 99th percentile upper reference limit of the Elecsys Troponin T assay were 5 ng/L and 14 ng/L, respectively [11].
4. Statistical Analyses
The study population was divided into two groups according to their cTnT levels: elevated (>14 ng/L) and normal (≤14 ng/L). Continuous variables were expressed as the mean±standard deviation or median [first quartile; third quartile] and were compared using the Student's t-test or the Mann–Whitney U test. Categorical variables were compared using the χ2 test or Fisher's exact test. Univariate and multivariate Cox proportional hazards regression analyses were performed to assess the association between the clinical or laboratory variables and the 30-day all-cause mortality of patients with stroke. The hazard ratio (HR) and 95% confidence interval (CI) of the HR were calculated. The Kaplan–Meier method and log-rank test were used to compare the overall survival rates of patients in the elevated and normal cTnT level groups. Statistical analyses were performed using SPSS, version 18 for Windows (SPSS, Inc., Chicago, IL, USA). A probability value (P value) <0.05 was considered to indicate statistical significance.
RESULTS
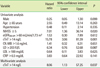
The mean age of the study population (182 patients) was 64.6±13.1 yr; 111 patients (61.0%) were male. Elevated cTnT levels were identified in 14.8% (27/182) of the patients with acute ischemic stroke. The median [first quartile; third quartile] cTnT values of the normal and elevated cTnT level groups were 7 ng/L [5; 10 ng/L] and 17 ng/L [16; 38 ng/L], respectively. The clinical and laboratory characteristics of the patients in this study are summarized in Table 1.
Patients with elevated cTnT levels were significantly older than those with normal cTnT levels (mean age, 74.7±12.2 vs. 62.9±12.4 yr; P<0.001) and were more likely to have a medical history of hypertension (P=0.044). The elevated cTnT level group also had more severe neurological deficits (based on NIHSS scores) than the normal cTnT level group (median [first quartile; third quartile] of the NIHSS score, 5.5 [3.0; 18.5] vs. 3.0 [1.0; 7.0], P=0.022; mRS score, 3.0 [1.0; 5.0] vs. 1.0 [1.0; 2.0], P<0.001) (Table 1).
Seven patients (3.8%) died during the follow-up period. Among the patients with acute ischemic stroke, all-cause mortality after 30 days differed significantly between the normal (1.3%, 2/155) and the elevated (18.5%, 5/27) cTnT level groups. In a univariate regression analysis, the NIHSS score (0–4 vs. ≥5) and the cTnT levels (≤14 vs. >14 ng/L) were associated with 30-day all-cause mortality. The HRs (95% CI) for the NIHSS score and cTnT levels were 7.01 (1.36–36.14) and 15.78 (3.06–813.9), respectively. A multivariate Cox proportional hazards regression analysis considering sex, age, history of hypertension, NIHSS score, mRS score, LD, LDL, eGFR, CRP, FDP, CK-MB, and cTnT showed that only the cTnT level was an independent predictor of 30-day all-cause mortality in patients with acute ischemic stroke (HR 8.06, 95% CI 1.13–57.25, P=0.037) (Table 2).
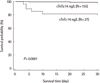
The Kaplan–Meier survival analysis revealed a significantly higher survival rate in patients in the normal cTnT level group than those in the elevated cTnT level group (P<0.0001) (Fig. 2).
DISCUSSION
Elevated cTnT levels have been reported in 0–36% of patients with acute ischemic stroke [481213]. However, these studies describing the relationship between cTnT levels and acute ischemic stroke were highly heterogeneous. Furthermore, it is difficult to compare their results directly due to differences in the study setting, troponin assays, and cutoff values. In our study on patients with acute ischemic stroke, the frequency of cTnT elevation in the study population was 14.8%, which was consistent with the rates determined in earlier studies.
The etiology and mechanism of the increase in cTnT level in patients with acute stroke have been debated. The associated myocardial damage and elevated cTnT level after acute ischemic stroke have been attributed to a variety of causes [1415], including the coexistence of acute cerebral ischemia with ischemic myocardial necrosis [14]. Alternatively, congestive heart failure and renal insufficiency, rather than myocardial infarction, have been cited as being responsible for the elevated cTnT levels [16]. Barber et al. found that increased serum troponin after acute ischemic stroke was associated with elevated circulating levels of epinephrine, consistent with the activation of the sympathetic nervous system [8]. Another study reported elevated serum cortisol levels after stroke, and the association of higher concentrations in patients with myocardial damage [17]. Increased catecholamine release has also been proposed to cause the excessive release of intracellular calcium ions, thereby causing myocyte dysfunction [18]. These findings suggest that a relationship exists between the sympathetic nervous system and myocardial cell damage in ischemic stroke patients. In this study, although efforts were made to exclude patients with concurrent acute coronary syndrome, acute ischemic stroke, and abnormal electrocardiography or echocardiography findings, these features could not be clearly distinguished in the patients in this study, nor did we assess their hormonal status.
In our patients with acute ischemic stroke, cTnT elevation had a significant prognostic impact. The HR for 30-day all-cause mortality in patients with an elevated vs. patients with normal cTnT level was 8.06 (95% CI, 1.13–57.25, P=0.037), according to a multivariate Cox proportional hazards regression analysis. Other large-scale and well-designed prospective studies have concluded that in the general population, a higher cTnT level was a strong risk marker for acute ischemic stroke [1920]. Increased levels of cTnT are associated with major adverse cardiac events and even mortality from non-cardiovascular causes. Moreover, a prospective trial found that the cTnT level was the strongest predictor of vascular events and all-cause mortality in patients with acute cerebral ischemia; in a multivariate analysis, it was the only marker that remain ed signifi-cantly predictive [14]. These findings from earlier studies together with the results of this study reinforce the prognostic association between elevated cTnT levels and ischemic stroke.
There were several limitations to our investigation. First, we relied on a single measurement of serum cTnT rather than serial serum cTnT changes, which might have provided additional information for the diagnosis of acute myocardial infarction. Second, our study was retrospective rather than prospective; consequently, the method of data collection may have undermined the appropriate interpretation of the results. Finally, we only evaluated all-cause mortality, not specific causes of death.
In conclusion, our findings contribute to an improved understanding of the implications of serum cTnT elevation in patients with acute ischemic stroke. A systematic study performed in a larger cohort with a long-term follow-up of patients with acute ischemic stroke is necessary to clarify the clinical significance of elevated cTnT levels in this population. Nonetheless, clinicians should consider measuring serum cTnT concentration routinely in patients with acute ischemic stroke, which may help them in making a predictive prognosis.


 XML Download
XML Download