

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background
Throat culture is the golden standard for diagnosis of group A streptococcal (GAS) pharyngitis. However, because it is a time-consuming procedure, antibiotics are often empirically administrated. Rapid antigen tests (RATs) can detect bacterial infections within 15 minutes, thus helping to reduce unnecessary administration of antibiotics.
Methods
In total, 108 patients, between 3 and 17 yr of age, who visited our hospital from August 2011 to July 2012, were tested for suspected acute pharyngitis with two RATs––SD Bioline Strep A (SD, Korea) and BinaxNOW Strep A (Binax, Inc., USA)––as well as throat culture. We compared the sensitivity, specificity, and consistency of the two RATs and assessed the clinical manifestations of GAS pharyngitis.
Results
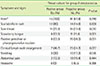
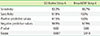
Of the 108 patients, 15 were confirmed to have GAS pharyngitis by throat culture. The SD test showed a sensitivity of 93.3% and a specificity of 97.8%; the positive and negative predictive values were 87.5% and 98.9%, respectively. The Binax test showed a sensitivity of 86.7% and a specificity of 100%; the positive and negative predictive values were 100% and 97.9%, respectively. The Kappa values for conformity degree were high, 0.887 and 0.918 in the SD and the Binax tests, respectively (P=0.00). Clinical manifestation assessment of GAS pharyngitis indicated that scarlatiniform rash and strawberry tongue were significantly associated signs (P<0.05).
Figures and Tables
Table 1
Symptoms and signs of acute pharyngitis
![]()
Table 2
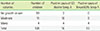
Comparison of rapid antigen detection test results based on the number of colonies of group A streptococcus in throat culture
| Number of colonies | Number of children | Positive cases of SD Bioline Strep A | Positive cases of BinaxNOW Strep A |
|---|---|---|---|
| No growth or rare | 93 | 2 | 0 |
| Moderate | 11 | 10 | 9 |
| Many | 4 | 4 | 4 |
| Total | 108 | 16 | 13 |
![]()
References
1. Dimatteo LA, Lowenstein SR, Brimhall B, Reiquam W, Gonzales R. The relationship between the clinical features of pharyngitis and the sensitivity of a rapid antigen test: evidence of spectrum bias. Ann Emerg Med. 2001; 38:648–652.

2. Nelson JD. The effect of penicillin therapy on the symptoms and signs of streptococcal pharyngitis. Pediatr Infect Dis. 1984; 3:10–13.
3. Kelly MT, Smith JA, Jaffer S, Pearce L, Clarke A. Outpatient evaluation of a rapid, direct test for detection of group A streptococci in throat swabs. Am J Clin Pathol. 1987; 87:522–525.
4. Redd SC, Facklam RR, Collin S, Cohen ML. Rapid group A streptococcal antigen detection kit: effect on antimicrobial therapy for acute pharyngitis. Pediatrics. 1988; 82:576–581.
5. Bisno AL, Gerber MA, Gwaltney JM Jr, Kaplan EL, Schwartz RH. Infectious Diseases Society of America. Practice guidelines for the diagnosis and management of group A streptococcal pharyngitis. Clin Infect Dis. 2002; 35:113–125.
6. Breese BB. A simple scorecard for the tentative diagnosis of streptococcal pharyngitis. Am J Dis Child. 1977; 131:514–517.
7. Pickering LK, Baker CJ, Kimberlin DW, Long SS, editors. Red Book: 2009 Report of the Committee on Infectious Diseases. 28th ed. Elk Grove Village, IL: American Academy of Pediatrics;2009. p. 619.
8. Shin YJ, Jang SH, Dong ES, Ahn YM, Ku MS. Clinical manifestations of group A β-hemolytic streptococcal pharyngits and usefulness of rapid antigen test. Korean J Pediatr. 2001; 44:732–741.
9. Kim JM. National survey on the current status of antibiotic use in Korea and a proposition on the appropriate use of antibiotics. J Korean Soc Chemother. 1999; 17:259–261.
10. Garcia LS. Clinical microbiology procedures handbook. 3rd ed. ASM press: American Society of Microbiology;2010. p. 3.11.2.9–3.11.2.11.
11. Swartz B, Marcy M, Phillips WR, Gerber MA, Dowell SF. Pharyngitis—principles of judicious use of antimicrobial agents. Pediatrics. 1998; 101:171–174.
12. Kaplan EL, Johnson DR, Del Rosario MC, Horn DL. Susceptibility of group A beta-hemolytic streptococci to thirteen antibiotics: examination of 301 strains isolated in the United States between 1994 and 1997. Pediatr Infect Dis J. 1999; 18:1069–1072.
13. Jersild T. Penicillin therapy in scarlet fever and complicating otitis. Lancet. 1948; 1:671–673.
14. Gerber MA, Shulman ST. Rapid diagnosis of pharyngitis caused by group A streptococci. Clin Microbiol Rev. 2004; 17:571–580.
15. Mayes T, Pichichero ME. Are follow-up throat cultures necessary when rapid antigen detection tests are negative for group A streptococci? Clin pediatr (Phila). 2001; 40:191–195.
16. Bisno AL, Peter GS, Kaplan EL. Diagnosis of strep throat in adults: are clinical criteria really good enough? Clin Infect Dis. 2002; 35:126–129.
17. Song SK, Hong MA, Oh KC, Ahn SI, Tae MH, Shin HJ, et al. Comparison of two rapid antigen detection tests for diagnosis of group A streptococcal pharyngotonsillitis. J Korean Pediatr Soc. 2002; 45:973–979.
18. Lim KH, Choi WJ, Kim MJ, Kim YH, Jung JA, Yang S, et al. Utility of streptococcal rapid antigen detection test in children with acute pharyngitis. Pediatr Allergy Respir Dis. 2006; 16:57–65.
19. Al-Najjar FY, Uduman SA. Clinical utility of a new rapid test for the detection of group A streptococcus and discriminate use of antibiotics for bacterial pharyngitis in an outpatient setting. Int J Infect Dis. 2008; 12:308–311.
20. Gerber MA. Diagnosis and treatment of pharyngitis in children. Pediatr Clin North Am. 2005; 52:729–747.
21. Hsieh TH, Chen PY, Huang FL, Wang JD, Wang LC, Lin HK, et al. Are empiric antibiotics for acute exudative tonsillitis needed in children? J Microbiol Immunol Infect. 2011; 44:328–332.
22. Putto A. Febrile exudative tonsillitis: viral or streptococcal? Pediatrics. 1987; 80:6–12.
 XML Download
XML Download