

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Diabetes mellitus (DM) is a metabolic disease that is caused by defects in insulin secretion or peripheral resistance of the tissues to insulin. A chronic hyperglycemic state damages the organs, including the vessels, eyes, kidneys, nerves, and heart, and can ultimately cause complex organ failure [1]. The prevalence of DM is rapidly increasing, and the World Health Organization estimated that 330 million people would be diagnosed with diabetes by 2025 [2].
Hemoglobin A1c (HbA1c) is the most reliable indicator of long-term glycemic conditions and reflects the average blood glucose level in the past 2-3 months. The level of HbA1c is considered to decide on the best treatment for DM and to monitor and prevent diabetes-related complications [3]. An HbA1c level of ≥6.5% (48 mmol/mol) has recently been recommended by the as a diagnostic criterion for diabetes [4]. In addition, the Diabetes Control and Complications Trial (DCCT) established a standard value based on the National Glycohemoglobin Standardization Program (NGSP), which specifies a value of 6.5% as positive diagnosis of DM, while values ranging from 5.7-6.4% are considered as high risk for diabetes. HbA1c measurement via point-of-care testing (POCT) can shorten the report time without pre-treatment of the sample, such as transportation to a central laboratory and centrifugation after collection. POCT typically requires minimal personnel training and can be easily performed by doctors as well as nurses [56]. Based on the prompt return of the results, POCT is very convenient for patients, as it enables immediate treatment planning without additional clinic visits.
The LABGEO PT10 analyzer (Samsung Electronics, Suwon, Korea) is a POCT device used for clinical chemistry test items with good reported analytical performance [7]. LABGEO PT10 Hemoglobin A1c cartridges (Samsung Electronics) have recently been developed and can be used in diabetic care. In this study, we evaluated the difference in LABGEO PT10 HbA1c values in capillary blood, EDTA whole blood, and lithium (Li)-heparin whole blood. The HbA1c reference values were determined using a DCCT aligned cationic exchange high performance liquid chromatography (HPLC) analyzer.
MATERIALS AND METHODS
Study Design
This study was approved by the institutional review board of Samsung Medical Center. HbA1c values were measured in 76 individuals aged 23-82 yr (median 58 yr). Of the 76 participants, 41 (54%) were male and 35 (46%) were female. Several blood samples were collected from the volunteers simultaneously and were used for HbA1c testing. Capillary blood was collected in heparinized capillary tubes (Kimble Chase Life Science, Rockwood, TN, USA) from a finger prick and was tested using the LABGEO PT10. Venous blood was collected in a BD Vacutainer® K2 EDTA tube (BD Biosciences, Franklin Lakes, NJ, USA) and a BD Vacutainer® PST™ Gel and Lithium heparinN tube (BD Biosciences) and was analyzed using the LABGEO PT10 and Variant II Turbo HbA1c Analyzer (Bio-Rad Laboratories, Hercules, CA, USA). A duplicate measurement for HbA1c was performed for all specimens and instruments.
HbA1c values were compared according to the sample type and by following Clinical and Laboratory Standards Institute Guidelines for EP9-A3 [8] and EP14-A2 [9]. Values were compared using Passing-Bablok regression and Bland-Altman plots. Cohen's kappa (κ) values were used to estimate concordance between the assays, with values >0.81 considered excellent concordance, 0.80-0.61 considered good concordance, and 0.60-0.41 considered moderate concordance [10].
LABGEO PT10 Analyzer
The LABGEO PT10 analyzer was used in conjunction with the HbA1c cartridges. We used the same lot of cartridges and equipment throughout the evaluation period. The LABGEO PT10 weighs 2 kg and has dimensions of 140 mm (width)×206 mm (depth)×205 mm (height). The analyzer features a graphic color liquid crystal display module with a touch-screen and built-in thermal printer module. The analyzer operation requires minimal training of laboratory personnel. LABGEO PT10 HbA1c was measured using the latex bead agglutination method and the estimated average glucose value was calculated. The latex bead agglutination method for HbA1c is based on the interactions between antigen molecules (HbA1c) and HbA1c-specific antibodies coated on the latex beads. This cross-linking reaction alters the solution turbidity to an extent proportional to the amount of antigen in the samples.
The LABGEO PT10 was designed to function with ready-to-use cartridges, while a 7-minute analysis time is required to complete one test. The LABGEO PT10 can analyze HbA1c after loading the cartridge containing 1-µL whole blood and capillary blood samples. Test results were certified by the NGSP and were adjusted according to the DCCT guidelines.
Comparative Central Laboratory Method
The Variant II Turbo utilizes the boronate affinity HPLC method, which separates glycated hemoglobin from the non-glycated fraction. The standardized HbA1c value was calculated from the glycated hemoglobin result using an algorithm. Variant II Turbo is standardized to the International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) reference method and is traceable to DCCT and NGSP.
RESULTS
The central laboratory method results for the EDTA whole blood samples indicated that the range for the Variant II Turbo was 4.8-10.2% (median 6.3%) and the Li-heparin whole blood sample range for the Variant II Turbo was 4.8-9.9% (median 6.1%). All samples, including capillary blood, were appropriately distributed. The correlation coefficient (r) for capillary blood using the LABGEO PT10 vs. EDTA whole blood analysis using the Variant II Turbo was r=0.9619, and that of capillary blood using the LABGEO PT10 vs. Li-heparin whole blood analysis using the Variant II Turbo was r=0.9619 (Fig. 1).
Using the LABGEO PT10, the correlation coefficient was r=0.9697 for capillary blood vs. EDTA whole blood, r=0.9724 for capillary blood vs. Li-heparin whole blood, and r=0.9730 for EDTA whole blood vs. Li-heparin whole blood (Fig. 2).
The average HbA1c bias for each type of sample that was compared (with 95% confidence intervals in parentheses) as observed from the Bland-Altman plots was as follows: capillary blood by LABGEO PT10 vs. EDTA whole blood using the Variant II Turbo, -0.25% (-0.33–-0.17%); capillary blood by LABGEO PT10 vs. Li-heparin whole blood using the Variant II Turbo, -0.12% (-0.19–-0.04%); capillary blood using the LABGEO PT10 vs. EDTA whole blood using the LABGEO PT10, -0.14% (-0.20–-0.07%); capillary blood using the LABGEO PT10 vs. Li-heparin whole blood using the LABGEO PT10, -0.08% (-0.14–-0.01%); EDTA whole blood using the LABGEO PT10 vs. Li-heparin whole blood using the LABGEO PT10, -0.07% (-0.13–-0.002%).
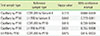
Cohen's kappa coefficient was calculated to assess the concordance between each instrument and between each sample type. Cohen' kappa (κ) values showed excellent concordance between capillary blood and EDTA whole blood (κ=0.816), capillary blood and Li-heparin whole blood (κ=0.831), and between EDTA whole blood and Li-heparin whole blood (κ=0.875) when HbA1c was determined based on the LABGEO PT10. The kappa (κ) values showed good agreement between the level of HbA1c in capillary blood based on the LABGEO PT10 and Li-heparin whole blood based on the Variant II Turbo (κ=0.842), and between capillary blood based on the LABGEO PT10 and EDTA whole blood based on the Variant II Turbo (κ=0.773) (Table 1).
DISCUSSION
Glycated hemoglobin measurement was introduced in clinical laboratories in approximately 1977, and numerous methods have been developed to measure glycated hemoglobin since this concept was introduced. Nearly all current methods evaluate the differences in charge (HPLC method) or structure (affinity chromatography or immunoassay) of glycated hemoglobin to measure HbA1c. Additionally, many HbA1c point-of-care instruments are used in diabetic care centers, including the DCA Vantage (Siemens Medical Solutions Diagnostics, Tarrytown, NY, USA), In2it (Bio-Rad, Hercules, CA, USA), and A1CNow (Bayer HealthCare, Sunnyvale, CA, USA). HbA1c is an important indicator for treating diabetes, and has recently been included in the standard of diagnosis for diabetes and for high-risk criteria [4]. The DCCT found that a 1% reduction in HbA1c levels resulted in a 43-45% reduced risk of diabetic retinopathy [1].
HbA1c laboratory measurement should be certified by the NGSP and measured using the DCCT reference method [4]. To obtain NGSP certification, laboratory methods should meet the NGSP criteria, in which at least 37 of 40 individual results are within 6% of an NGSP network laboratory for a method [11]. Additional representative reference methods for HbA1c include NGSP and IFCC. The NGSP method presents the result as a percentage, while the IFCC reference method is presented in mmol/mol. HbA1c values obtained using the IFCC method are 1.5-2% lower than the NGSP results. When the IFCC unit is reported, an equation can be used to convert the value to a relative NGSP value: NGSP %=[0.09148 × IFCC mmol/mol] + 2.152. In addition, a recent consensus recommends that the results be reported in both units [12].
In this study, we determined the HbA1c levels in three sample types and using two instruments. The results indicated that the correlation between LABGEO PT10 among capillary blood, EDTA whole blood, and Li-heparin whole blood was good (capillary blood vs. EDTA whole blood, r=0.9697; capillary blood vs. Li-heparin whole blood, r=0.9724; EDTA whole blood vs. Li-heparin whole blood, r=0.9730). Excellent concordance was observed between capillary blood and EDTA (κ=0.816), capillary blood and Li-heparin (κ=0.831), and EDTA blood and Li-heparin blood (κ=0.875). These findings suggest that the LABGEO PT10 can be used in various clinical environments to accurately determine the HbA1c levels.
Although good correlation was observed in the LABGEO PT10 testing of capillary blood, EDTA whole blood, and Li-heparin whole blood, there were some limitations to our study. In this study, the interference from hemoglobin variants was not evaluated. The difference in HbA1c values from the variant hemoglobin is an important parameter for measuring HbA1c. The methods available for measuring HbA1c are diverse, and hemoglobin variants showing interference differ according to the type of measurement used [1314]. Although we were unable to assess the interference effect of variant hemoglobin, an immunoassay using same principle as LABGEO PT10 is known as be affected by HbS or HbC, but not by HbE or HbD [13]. Interference can occur when using antibodies that are specific to the glycated N-terminal amino acid of HbA1c. Since the HbS and HbC are close to the N-terminus on the β chain, making them distinct form HbE or HbD, some immunoassays are affected by the presence of these variants.
The LABGEO PT10 is a small and lightweight device that can be used directly onsite. It can be used to analyze HbA1c using whole blood or capillary samples. This equipment can be managed easily, and a quality control mode or self-diagnostic mode is included. A previous study reported a strong correlation between the LABGEO PT10 and Integra 800 immunoassay (correlation coefficient r=0.9843, slope of 1.054, and Y intercept of -0.468). The LABGEO PT10 showed a linear association in the clinically important application range of 3.95-12.36% (R2=0.9968, slope of 1.001, and Y intercept of -0.198) and total coefficients of variation were between 3.8% and 4.2% [7]. In HbA1c measurement, it is recommended that intralaboratory coefficient of variation <2% and an interlaboratory coefficient of variation <3.5% [15]. However, meeting this stringent criterion is very difficult, and it seems inappropriate to impose this goal on POCT devices [16].
However, previous studies did not compare sample types such as EDTA whole blood and capillary blood. In this study, we evaluated HbA1c values in three types of samples (capillary blood, EDTA whole blood, and Li-heparin whole blood). Various HbA1c levels were included in the comparison analysis and good correlation and concordance were observed among the three types of blood samples using the two different analytical instruments.
In conclusion, the LABGEO PT10 can rapidly measure HbA1c under various sample conditions. No previous studies have compared HbA1c values based on sample types. Because measurement of HbA1c by the LABGEO PT10 provided immediate results, it is very convenient for patients who are unable to take venipuncture or cannot revisit medical centers with low accessibility, such as remote rural communities, primary healthcare, and outpatient clinics.
Measurement of HbA1c using the LABGEO PT10 produces immediate results, which is very convenient for patients. Finally, based on these results, the measurement of HbA1c in capillary blood showed results that were comparable to results from WB samples. The LABGEO PT10 can also be used for patients who are reluctant to undergo venipuncture.


 XML Download
XML Download