

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Eggerthella lenta is part of the normal human intestinal flora and has been most commonly associated with infections arising from the gastrointestinal tract [1]. Predisposing conditions include gastrointestinal tract disease, malignancies, hepatobiliary disease, immobilization, bedsores, diabetes mellitus, and stroke [234]. E. lenta is an emerging pathogen that has been under-recognized because of difficulties with its laboratory identification [3]. Few reports have addressed E. lenta infections or optimal treatments thereof. Here, we describe one case that we treated and briefly summarize the available data on E. lenta bacteremia.
CASE REPORT
A 73-yr-old male presented with fever, vomiting, and dyspnea. His medical history included a prior cerebrovascular attack and multiple complications caused by hemiplegia, including recurrent urinary tract infections and pressure sores requiring continuous medical care.
On the day of admission, his body temperature, pulse rate, respiratory rate, and blood pressure were 40.4℃, 108/min, 39/min, and 170/90 mmHg, respectively. Abdominal examina-tion revealed diffuse tenderness and guarding with absence of bowel sounds. The initial laboratory test data were as follows: Hb, 14.9 g/dL; white blood cell count, 7,250/µL (neutrophils, 78.0%); and platelets, 110,000/µL. His procalcitonin level was elevated to 28.46 ng/mL. Sputum and urine cultures were negative. PCR to detect Mycobacterium tuberculosis was negative. Abdominal and pelvic contrast computed tomography scans were suggestive of an abdominal abscess; air appeared to be present at the junction of the distal ileum and cecum. On admission, we ordered blood cultures to evaluate the fever. Escherichia coli was isolated, so we prescribed empirical intravenous levofloxacin. Despite 4 days of such treatment, the patient experienced fluctuating high-level fever, tachycardia, and hypotension and required intensive care. Blood was re-cultured and we additionally prescribed metronidazole. On hospital day 6, gram-positive rods were evident in an anaerobic blood culture bottle and were identified using several techniques, including Gram staining, examination of colony morphology, and VITEK 2 analysis (bioMérieux, Marcy, l'Etoile, France). The smooth gray colonies of rod-shaped non-sporulating bacteria were gram-positive, and the bacterial cells occurred either singly or in short chains. The isolate was catalase-positive and urease-negative. Glucose, galactose, maltose, sucrose, and saccharose were not fermented. VITEK MS (bioMérieux)-associated matrix-assisted laser desorption-ionization time-of-flight mass spectrometry identified E. lenta at a confidence level of 99.9%. For 16S rRNA sequencing, bacterial DNA was extracted, amplified, and sequenced with the aid of a 3,730 xL DNA Analyzer (sequencing service from Macrogen, Seoul, Korea). Comparison of the amplicon with database sequences (NCBI BLAST, Ez-Taxon database) revealed that the sequence was 99.9% (702/703 base pairs) identical to that of an authentic E. lenta strain (ATCC 25559). The minimum inhibitory concentrations of four antimicrobial agents were estimated using the Etest (bioMérieux), following the 2012 Clinical and Laboratory Standards Institute (CLSI) guideline M100-S22 [5]. The bacteria were grown on brucella agar supplemented with 5 µg/mL hemin, 1 µg/mL vitamin K1, and 5% (w/v) lysed sheep blood cells. The 2012 CLSI breakpoints [5] indicated that the isolate was susceptible to clindamycin, metronidazole, and meropenem, but resistant to ceftriaxone.
The fever and leukocytosis resolved slowly, and the patient was discharged after symptom relief. A nursing home stay was planned and follow-up outpatient visits were scheduled (Fig. 1).
DISCUSSION
E. lenta is an anaerobic, non-spore-forming, gram-positive bacillus of the Coriobacteriaceae first described in 1935 by Eggerth [6]. The bacterium was previously named Eubacterium lentum, but genetic analysis performed in 1999 showed that the bacterium merited its own genus [7]. Eggerthella and Eubacterium can be differentiated from closely related genera, including Propionibacterium, Bifidobacterium, Lactobacillus, and Actinomyces, on the basis of acid-production patterns upon growth in peptone/yeast extract/glucose broth. However, the bacteria are fastidious and slow-growing, and correct identification of E. lenta at the species level is difficult using conventional methods. Not even biochemical or fermentative reactions can reliably identify Eubacterium to the subspecies level [8].
Over the last decades, various commercial enzyme-based kits identifying clinically relevant anaerobes have been developed. These include the RapID-ANA II panel (Thermo Fisher Scientific Inc., Lenexa, KS, USA), the Minitek systems (BBL Microbiology Systems, Cockeysville, MD, USA), the Vitek Anaerobe Identification (ANI) card (bioMérieux), the BBL Crystal ANR ID kit (BD Diagnostics, Sparks Glencoe, MD, USA), and the API rapid ID 32A and API 20A systems (bioMérieux) [91011]. 16S rRNA sequencing is useful for confirming an E. lenta infection and is considered to be the gold standard [12]. Although we used the VITEK 2 ANI card, VITEK MS, and 16S rRNA sequencing, we suggest that the VITEK 2 system alone is adequate; the system is in use by many hospitals.
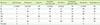
We reviewed 10 reports of laboratory-documented E. lenta bacteremia occurring from 2008 to 2015 (Table 1). Initially, traditional methods of bacterial identification (Gram staining, culture, and biochemical techniques) were used. Molecular techniques, including real-time PCR or microarray analysis, were secondarily employed to identify the causative organisms (71.4%). Many patients (81.0%) exhibited symptoms of gastroenteritis associated with diarrhea and/or vomiting. Abdominal pain was also often present. Those infected by E. lenta were already ill, and included patients hospitalized in intensive care units, the elderly, and patients with diabetes and/or chronic kidney failure (86.0%). Catheters (tubes inserted into blood vessels or the gallbladder) and other bodily tubes (e.g., running from the nose to the stomach) were common causes of bacteremia (19.0%). Several antimicrobial susceptibility testing methods (broth and agar dilution methods, disk-diffusion tests, the Etest, and automated testing systems) were used. The isolates were commonly susceptible to both clindamycin and metronidazole (Table 2).
In our case, E. coli was cultured from blood taken on the first day of hospitalization. Although we (empirically) prescribed levofloxacin, an intermittent fever (over 38.9℃) persisted for 4 days. On day 5, E. lenta was detected in the blood. After commencement of metronidazole, the fever slowly resolved. Because the isolate was resistant to levofloxacin but susceptible to metronidazole, we considered that the bacteremia was caused by a mixed infection of E. coli and E. lenta (the latter is not a normal component of skin flora). At the time of admission, the intra-abdominal abscess was the only obvious source of infection.
Recent reports have shown that several E. lenta infections were associated with the use of intrauterine devices, spondylodiscitis, female genital tract infections, cutaneous abscesses, and bacteremia (in Crohn's disease patients) [123412]. These data emphasize the importance of further investigation for bacterial virulence factors. It is suspected that transfer of E. lenta from an intra-abdominal abscess to the bloodstream may reflect a defect in the gastrointestinal tract; E. lenta is normally a gut commensal bacterium [1314]. Some reports found that E. lenta infection caused morbidity and mortality associated with septic shock and multiple organ failure. Although the pathogenesis of E. lenta bacteremia has not been well described [15], 10 recent reports indicate that the prognosis is rather favorable [12312151617181920]. Our patient required intensive care for several days but eventually recovered. Few data on E. lenta infections or the optimal treatment thereof are available.
In summary, we have reported a case of bacteremia caused by E. lenta in an elderly patient with an intra-abdominal abscess. We also reviewed the current literature.


 XML Download
XML Download