

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background
Anti-streptolysin O (ASO) test is usually used to diagnose group A streptococcal infection-related diseases, such as rheumatic fever, reactive arthritis, and various infectious diseases. Despite the recent declining incidence of these diseases, ASO test is still frequently performed as a screening test to diagnose rheumatic diseases. This study re-evaluated the clinical usefulness of ASO test in systemic rheumatic diseases (SRD).
Methods
ASO tests was performed in 825 patients between April and October in 2010. ASO levels were compared between SRD and non-SRD groups of patients. The results of ASO, C-reactive protein (CRP), and rheumatoid factor (RF) were compared among 6 subgroups of SRD: rheumatoid arthritis, systemic lupus erythematosus, ankylosing spondylitis, Behçet disease, Sjögren's syndrome and others.
Results
Positive results in ASO test (>200 IU/mL) were observed in 15.3% (126/825) of the patients tested. None of the ASO positive patients was, however, diagnosed with rheumatic fever or reactive arthritis. There were no statistically significant differences in the mean value (P=0.688) or positive rate (P=0.835) of ASO test between SRD and non-SRD groups. Positive rates of ASO test were also not statistically significant different among six subgroups of SRD patients (all P>0.05), whereas those of CRP and RF tests were significantly different.
Figures and Tables
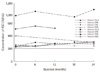 | Fig. 1Changes of ASO levels for 24 months in patients with systemic rheumatic diseases showing positive result at first visit.
Abbreviations: See Table 2.
|
Table 1
Comparison of ASO test in patients with systemic rheumatic diseases and non-systemic rheumatic diseases

![]()
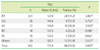
Table 3
P values in six subgroups of systemic rheumatic diseases for ASO, CRP, and RF test
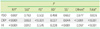
*P values by chi-square test; †P values by Fisher's exact test.
Abbreviations: CRP, C-reactive protein; RF, rheumatoid factor; others, See Table 2.
![]()
References
1. Shulman ST, Tanz RR. Group A streptococcal pharyngitis and immune-mediated complications: from diagnosis to management. Expert Rev Anti Infect Ther. 2010. 8:137–150.

2. Carapetis JR, McDonald M, Wilson NJ. Acute rheumatic fever. Lancet. 2005. 366:155–168.
3. Logan D, McKee PJ. Poststreptococcal reactive arthritis. J am Podiatr Med Assoc. 2006. 96:362–366.
4. Moorthy LN, Gaur S, Peterson MG, Landa YF, Tandon M, Lehman TJ. Poststreptococcal reactive arthritis in children: a retrospective study. Clin Pediatr (Phila). 2009. 48:174–182.
5. Brahmadathan KN, Gladstone P. Microbiological diagnosis of streptococcal pharyngitis: lacunae and their implications. Indian J Med Microbiol. 2006. 24:92–96.
6. Jansen TL, Janssen M, de Jong AJ, Jeurissen ME. Post-streptococcal reactive arthritis: a clinical and serological description, revealing its distinction from acute rheumatic fever. J Intern Med. 1999. 245:261–267.
7. Robertson KA, Volmink JA, Mayosi BM. Antibiotics for the primary prevention of acute rheumatic fever: a meta-analysis. BMC Cardiovasc Disord. 2005. 5:11.
8. Steer AC, Carapetis JR. Prevention and treatment of rheumatic heart disease in the developing world. Nat Rev Cardiol. 2009. 6:689–698.
9. Inglis TJ. Decline in rheumatic fever. Lancet. 1985. 2:1005–1006.
10. Jose VJ, Gomathi M. Declining prevalence of rheumatic heart disease in rural schoolchildren in India: 2001-2002. Indian Heart J. 2003. 55:158–160.
11. Olguntürk R, Aydin GB, Tunaoğlu FS, Akalin N. Rheumatic heart disease prevalence among schoolchildren in Ankara, Turkey. Turk J Pediatr. 1999. 41:201–206.
12. Visser H, Speyer I, Ozcan B, Breedveld FC, van Ogtrop ML, Hazes JM. The diagnostic value of streptococcal serology in early arthritis: a prospective cohort study. Rheumatology. 2000. 39:1351–1356.
13. Waits JB. Rational use of laboratory testing in the initial evaluation of soft tissue and joint complaints. Prim Care. 2010. 37:673–689.
14. Omurzakova NA, Yamano Y, Saatova GM, Mirzakhanova MI, Shukurova SM, Kydyralieva RB, et al. High incidence of rheumatic fever and rheumatic heart disease in the republics of Central Asia. Int J Rheum Dis. 2009. 12:79–83.
15. Veasy LG, Wiedmeier SE, Orsmond GS, Ruttenberg HD, Boucek MM, Roth SJ, et al. Resurgence of acute rheumatic fever in the intermountain area of the United States. N Engl J Med. 1987. 316:421–427.
16. Danchin MH, Carlin JB, Devenish W, Nolan TM, Carapetis JR. New normal ranges of antistreptolysin O and antideoxyribonuclease B titres for Australian children. J Paediatr Child Health. 2005. 41:583–586.
17. Ayoub EM, Nelson B, Shulman ST, Barrett DJ, Campbell JD, Armstrong G, et al. Group A streptococcal antibodies in subjects with or without rheumatic fever in areas with high or low incidences of rheumatic fever. Clin Diagn Lab Immunol. 2003. 10:886–890.
18. Cha SH, Choi YM, Yang SW, Lee DH, Lee CG, Hong CH. Upper limit of normal value for antistreptolysin O titer of healthy children in Seoul. J Korean Pediatr Soc. 1995. 38:1061–1068.
 XML Download
XML Download