

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Co-induction often has been used in clinical anesthesia as a method using two or more drugs during anesthesia induction.123 Theoretically, by using the drug combination with synergistic effect that produces an effect greater than the sum of their individual effects, anesthesia induction could be conducted with a reduced amount of each drug and therefore, we could expect the reduced occurrence of side effects.
Propofol and midazolam is a drug commonly used as sedative and hypnotics during anesthesia induction. Both drugs have a known synergistic hypnotic effect with each other, and co-induction with both drugs is a commonly used method for induction of anesthesia.12 Using synergistic hypnotic effect of propofol and midazolam, there were several research for the impact on the quality of anesthesia and cardiovascular in the variety age groups by midazolam with reduced induction dose of propofol required.34 However, there is no report on the effect of midazolam and propofol co-induction on hemodynamic responses in hypertensive patients who have fluctuating hemodynamic responses to tracheal intubation and on the reduction of complications such as hypotension by reducing the induction dose of propofol.56 Also, co-induction using a combination of three drugs, including an opioid which are widely used in the recent induction of anesthesia, has not yet been studied on the effect of hemodynamics in hypertensive patients.
Thus, this study evaluates the hemodynamic effects of co-induction with midazolam and propofol during remifentanil infusion and the effect of site target concentration in patients with hypertension. The results were compared to the hemodynamic effects of propofol induction alone during remifentanil infusion.
MATERIALS AND METHODS
The Institutional Ethics Committee approved this study, and written informed consent was obtained from all patients. Among patients who were scheduled for elective general, ENT, and gynecology surgeries under general anesthesia, this study enrolled 76 hypertensive patients who were American Society of Anesthesiologists physical status I-II, 30-65 years old, and had taken anti-hypertensive drugs for more than six months. Using a random number generated by the computer (computer-generated random numbers), patients were divided into midazolam-propofol (group MP, n = 38) and propofol (group P, n = 38) groups according to midazolam administration. Patients were excluded if they were obese (body mass index > 30), were expected to have difficult intubations, or if they had a history of myocardial infarction, congestive heart failure, chronic respiratory insufficiency (asthma or reactive airway), or diabetes.
Patients fasted for at least 8 hours before surgery. Antihypertensive drugs were taken with a small amount of water in the morning on the day of surgery, and no patients received other premedication.
On arriving to the operating room, standard monitoring including electrocardiogram, pulse oximetry, non-invasive blood pressure monitor, and bispectral index was applied to patient. Peripheral oxygen saturation, blood pressure (BP), and bispectral index (BIS) values were measured continuously or at regular intervals.
At 10 minutes before anesthesia induction, 5 ml/kg Ringer's lactate solution was administrated. Patients took deep breaths with 100% oxygen for 1 minute to allow preoxygentation. Glycopyrrolate 0.2 ㎎ i.v. bolus was administrated. For anesthesia induction, the co-induction group (group MP) received midazolam 0.03 ㎎/㎏. After 2 minutes, propofol 1.0 ㎎/㎏ i.v. bolus was administered over a period of 30 seconds. The propofol induction group (group P) received normal saline 0.03 ㎖l/㎏ instead of midazolam, and propofol 1.5 ㎎/㎏ i.v. bolus was administered over a period of 30 seconds. Remifentanil (UltivaTM inj., GlaxoSmithKline, Belgium) was administered simultaneously with propofol using a target control infusion pump syringe (Base Primea, Orchestra®, Fresenius Vial, France) at 4 ng/㎖ as the effect-site concentration. Minto's pharmacokinetic model was used to adjust the effect site target concentration.7 Two minutes after remifentanil infusion, 0.8 ㎎/㎏ rocuronium was administered for tracheal intubation and patients were intubated after 90 sec.
After intubation, anesthesia was maintained with effect site target concentrations of remifentanil 2 ng/㎖, sevoflurane 1.5%, oxygen 1.5 L/min, and air 2.5 L/min. Mechanical ventilation was started with tidal volume of 8 ㎖/㎏ and respiratory rate of 12/min, and was maintained with 30-35 mmHg of end tidal carbon dioxide. After that, patients did not receive any stimuli until the study was completed.
Two anesthesiologists who were unaware of patient groupings performed anesthesia induction. A skilled anesthesiologist performed endotracheal intubation, and another anesthesiologist recorded systolic, diastolic, and mean blood pressure (SBP, DBP, and MBP) and heart rate (HR) measurements. Another anesthesiologist who was not involved in anesthesia prepared experimental drugs and the propofol syringe was wrapped with white tape to hide the dose difference between groups. A nurse who was unaware of patient groupings injected the drugs under direction from an anesthesiologist.
The time from propofol administration to loss of consciousness (patients stop responding to the oral command “Look out of your eye” or had loss of eyelid reflection) and BIS value at loss of consciousness were measured. SBP, DBP, MBP, and HR were measured and recorded at before anesthesia induction (B0), 2 minutes after midazolam or saline administration (B1), 2 minutes after propofol administration (B2), 1 minute after rocuronium administration (B3), and immediately, 1, 2, and 3 minutes after intubation (T0, T1, T2, T3).
Rescue medication (concentration of sevoflurane administration was increased form 1.5% to 2.5%) was administered for patients with hypertension (SBP > 200 mmHg or more than 30% increase above baseline value). If SBP decreased 30% below baseline or to less than 80 mmHg, ephedrine 5 ㎎ was administered. When HR was less than 45 beats/min, 0.5 ㎎ atropine was administered intravenously.
To detect a 10% difference in mean blood pressure due to endotracheal intubation, 34 people per group were required for a power analysis of 0.8 (α = 0.05, β = 0.2). With anticipation of dropout, this study included 38 patients per group, with a total of 76 patients.
Statistical analysis was performed with SPSS (version 18.0, SPSS Inc., Chicago, USA). The Shapiro-Wilk test was used to test the normal distribution of continuous variables. Groups of data that follow a normal distribution were compared using a two tailed unpaired, student t-test, and values are expressed as mean and standard deviation. Categorical data were analyzed using the Chi-square test or Fisher exact test. Repeated-measures analysis of variance with correction by the Bonferroni method for multiple comparisons was used to evaluate changes in BP, HR, and BIS between and within groups. P values less than 0.05 were considered statistically significant.
RESULTS
There were no significant differences between the two groups in age, gender, weight, height (Table 1), and anti-hypertensive medication (Table 2). SBP, DBP, MBP, and HR before induction of anesthesia (B0) also did not differ between the two groups (Table 1).
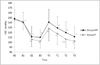
After anesthesia induction, SBP decreased compared to before induction (B0) in both groups. SBP of the group P was significantly decreased from propofol administration (B2) to 3 minutes after intubation (T3). The SBP of the group MP was also significantly reduced at all time points, except for immediately after extubation (T0) (Fig. 1).
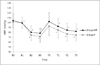
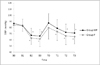
Comparison of the groups showed that the SBP of the group MP was high compared to that of between groups immediately after intubation (T0). After intubation, the SBP of the group MP was also higher than that of the group P until 3 minutes after intubation (T3). There was no significant difference between the groups except at 2 minutes after intubation (T2) (P < 0.05) (Fig. 1). The decreases in DBP and MBP in the group MP were smaller than those of the group P from propofol administration (B2) to 3 minutes after intubation (T3). However, there was no significant difference between groups (Fig. 2 and 3).
In both groups, HR significantly decreased after propofol administration (B2) compared to before anesthesia induction (B0). After intubation (T0), HR significantly increased compared to before anesthesia induction (B0) in both groups. However, there were no significant differences between groups (Fig. 4).
Ephedrine (5 ㎎) was administrated as a rescue treatment for decreased systolic BP to 5 patients in the group MP and 12 cases in the group P. However, there were no significant differences between groups (P = 0.1).
One patient in each group needed increased sevoflurane concentration due to increased BP after tracheal intubation. HR less than 45 beats/min did not occur in either group.
The group MP took 50 ± 8 seconds to lose consciousness while the group P took 52 ± 13 seconds, and there was no significant difference between the two groups. The BIS value at loss of consciousness (group MP 78 ± 6, group P 80 ± 9) was also not significantly different between groups.
DISCUSSION
The results of this study show that midazolam 0.03 ㎎/㎏-propofol 1.0 ㎎/㎏ co-induction with 4 ng/㎖ remifentanil effect site concentrations suppress excessive hemodynamic responses during intubation and induction in hypertensive patients. The propofol induction with remifentanil group showed a lower SBP than the midazolam-propofol co-induction with remifentanil group. However, there was no significant difference between groups except for at 2 minutes after intubation. These results are similar to those of previous studies that midazolam-propofol co-induction significantly reduced the requirement dose of propofol through a synergistic hypnotic effect, but did not show a significant difference in cardiovascular response when compared with propofol induction.12
Anesthesia co-induction with two or more drugs acts through an added effect (additive interaction) or synergism (synergistic interaction) between the combined drugs. Reduced drug side effects are expected because decreased amounts of each drug are used at the same time.8 Several studies have investigated hemodynamic effects during anesthesia induction using various combinations of midazolam, propofol, and opioid formulations in different age groups. Win et al.9 reported that when they induced anesthesia in adult patients using midazolam-propofol co-induction, the baroreflex mechanism of the autonomic nervous system was well maintained. However, when propofol alone was used for anesthesia induction, the baroreflex mechanism of the autonomic nervous system was reduced, as was cardiac output index. Thus, they reported that co-induction resulted in a more stable cardiovascular response than administration of propofol alone during anesthesia induction and intubation. However, another study reported that anesthesia induction with fentanyl added to midazolam and propofol co-induction does not show the same benefits on cardiovascular stability in elderly and young adults. Instead, this protocol temporarily reduced SBP and BMP in patients 60 years of age or older.3 Like this, a variety of co-induction methods may affect various hemodynamic responses during anesthesia induction and the hemodynamic response depends on the amount of drug that is used as well as which drugs are used.
This study reduced propofol dosage to 0.5 ㎎/㎏ (1.5 ㎎/㎏ to 1.0 ㎎/㎏) with midazolam 0.03 ㎎/㎏. Lee et al.10 reported that propofol effect site target concentration of 4 ug/㎖ and remifentanil effect site target concentration of 4 ng/㎖ can effectively reduce the cardiovascular response to laryngoscope and endotracheal intubation during anesthesia induction in hypertensive patients. By refer that 1.43 ㎎/㎏ of propofol was administered until the patient's loss of consciousness, 1.5 ㎎/㎏ of propofol i.v. bolus was determined for anesthesia induction. In addition, based on another study that, when using the midazolam 0.025 to 0.05 ㎎/㎏ in the younger and older adults, there was a greater percentage reduction (22 - 52%) in induction dose requirements of propofol.311 Although, propofol is a drug widely used during anesthesia induction, propofol reduces BP in proportion to dosage and plasma concentration. This reduction in BP was related to decrease in systemic vascular resistance and cardiac output.1213 We hypothesized that BP changes in the two groups would differ during anesthesia induction because of the different propofol dosages administered. In this study, the width of BP reduction was small in the co-induction group compared to the propofol alone group. However, there was no statistically significant difference between groups. This indicates that different propofol dosages between the two groups did not significantly affect hemodynamic responses in the present study.
Remifentanil was also used in addition to midazolam and propofol in this study. Because remifentanil acts very quickly from the onset and has a short half-life of 1-2 minutes, it is widely used during anesthesia induction. It might be helpful in suppressing the cardiovascular response to transient stimuli such as endotracheal intubation.1415 Combinations of short-acting opioids, such as remifentanil and propofol have been widely used to effectively suppress BP increases in both normotensive and hypertensive patients during anesthesia induction.1617 Because propofol reduces BP in proportion to dosage, a combination of two drugs may cause unwanted reactions such as severe hypotension and bradycardia.18 In this study, rescue therapy was necessary for one patient in each group due to increases in BP during induction. Whereas, ephedrine was administrated to five patients in the group MP and 12 patients in the group P due to decreases in BP. Maguire et al.19 also reported that anesthesia induction with remifentanil and propofol effectively suppresses BP in hypertensive patients. However, rescue therapy was also needed (systolic arterial pressure below 100 mmHg prior to induction or reduction of more than 30%) for 7 of 20 patients due to reduced BP after intubation. Similarly, the results of this study suggest that induction with remifentanil 4 ng/㎖ effectively suppresses BP increases in hypertensive patients immediately after intubation. However, there is potential to increase BP regardless of whether propofol alone or midazolam-propofol co-induction is used. Thus, the possibility of lowering blood pressure as well as rising blood pressure should be considered during anesthesia induction in hypertensive patients. As well as sufficient fluids administration, anesthesiologist checks the appropriate doses of blood pressure medication before anesthesia induction to prevent sudden changes in blood pressure. Depending on the situation, anesthesiologist will need immediate treatment by using the appropriate emergency medicine such as vasopressor or ephedrine.
In this study, the midazolam-propofol co-induction group had similar BIS values at loss of consciousness and time required to unconsciousness as the propofol alone group. Although there were no significant differences in hemodynamic effects between the two groups, the drug administration method (propofol following 2 minutes after midazolam) and dosage used in this study allowed appropriate sedation and hypnotic effects during anesthesia induction. Thus, we think this method could be an alternative induction method for sedation and hypnotics in hypertensive patients.
A limitation of this study is that propofol was administered manually without the use of an infusion pump. Propofol infusion rate can impact cardiovascular effects.20 Therefore, it is important to maintain a constant speed of propofol administration using an infusion pump. Although propofol was administrated manually without an infusion pump, we had planned to minimize the cardiovascular effects of the infusion rate by using different injection times for each group. However, to avoid having the anesthesiologist know which group a patient belongs to, propofol was manually injected at the same time for 30 seconds in both groups. Another limitation of this study is that the effect of various remifentanil concentrations with midazolam-propofol co-induction was not further researched. In this study, remifentanil was administrated using a target effect site concentration method based on body weight, age, and height instead of only weight.21 Further research about the hemodynamic effects of midazolam-propofol co-induction with slightly reduced or different remifentanil concentrations is needed.
Midazolam 0.03 ㎎/㎏-propofol 1.0 ㎎/㎏ co-induction with 4 ng/㎖ of remifentanil TCI has similar effect to propofol 1.5 ㎎/㎏ with remifentanil TCI in attenuating increased BP and HR and inducing hypnosis during endotracheal intubation and anesthesia induction in hypertensive patients. This method could be alternative methods for preventing increased blood pressure during anesthesia induction and intubation in hypertensive patients.



 XML Download
XML Download