

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Diarrhea is a very common clinical symptom which is defined as feces containing water more than loose feces, passing stool more than 3 times a day due to the increase of water, amount or number of feces. Diarrhea for up to 14 days is classified as an acute diarrhea.4 One of the typical acute diarrheas is infectious diarrhea, which is caused by the infectious agent, and is accompanied by nausea, vomiting and abdominal pain.5 In case of advanced countries, viruses account for 30 to 40% of all cases of acute diarrhea.6 According to the report on the prevalence and characteristics of acute diarrheal diseases published by the Korea Centers for Disease Control and Prevention in 2008, the most common cause was Norovirus (28.8% of 8556 samples).7 In the acute diarrhea laboratory surveillance status published by the Korea Centers for Disease Control and Prevention in 2013, the virus detection rate was 29.9% and the bacteria detection rate was 17.62%.8
However, the results from these studies were mostly from sentinel surveillance projects, that included infants, children, healthy adults and the elderly. On the other hand, there were almost no investigations of immunocompromised patients for whom acute diarrhea can lead to death. In patients with HIV infection, solid tumor, hematologic malignancy, bone marrow or organ transplant, chronic diseases, and immunocompromised patients caused by chemotherapy and immunosuppressant, acute or chronic diarrhea is a serious complication.9 In other studies, C. difficile enteritis was common in immunocompromised hosts, but there was no comparison to the prevalence of other pathogens or non-infectious causes.10 C. difficile-associated disease (CDAD) causes diarrhea by damaging the intestinal mucous membrane through excessive proliferation of pre-existing or newly acquired C. difficile. The risk factors of CDAD are old age, long-term hospitalization, recent history of using antibiotics or proton pump inhibitor or immunocompromised patients who received chemotherapy or transplant, and patients who underwent gastrointestinal surgery.11 CDAD exhibited an incidence of 30 to 40 cases per 100,000 people in the USA and other countries until 1990s, but starting in the 2000s its incidence dramatically increased 2 to 3-fold. Recently, a sporadic epidemic of a hypervirulent strain, NAP1/027, which leads to fulminant colitis and eventually death was reported in the USA, Canada, Europe and Korea.12 In Korean CDAD studies, CDAD was observed in the community and as a hospital acquired infection, and it had been reported that it could have severe clinical effects, showing that the epidemiology of CDAD has changed. Therefore, studies and measures for this are needed.13
Common complications of acute diarrhea may include dehydration, acute renal failure which requires dialysis, severe malnutrition, intestinal perforation, and in severe cases, ventricular arrhythmia.2 In contrast, acute diarrhea in immunocompromised hosts (e.g., bone marrow transplant patients, organ transplant patients and chemotherapy patients) is commonly known to have severe effects requiring hospitalization, long exiting period of pathogen and ease of relapse.14 In the case of transplant patients, acute diarrhea is related to the loss of the transplanted organ and increased mortality and these results are known to be side effects of immunosuppresant use.15
For defining the immunocompromised host who is the subject of this study, “immunity” means the resistance to the infection and “compromised immunity” is deficiency in the defense mechanism against infection in a broad sense.16 The mechanism of immune deficiency can be classified as “primary” and “secondary”: primary immune deficiency is less frequent but the most common is IgA deficiency for which congenital phagocytosis activity and complement activity are the main actions.17 The causes of secondary immune deficiency include drug use such as steroids and immunosuppressants, diabetes, AIDS, tuberculosis, alcohol abuse patients, chronic renal failure, blood tumor disease (including leukopenia), and old age.16 In drug related cases, steroids are most common, and they reduce lymphocyte activity, the number and function of monocytes, inhibit opsonization, and cause the degradation of macrophage reaction to the T cell lymphokine.18 Considering the relationship between diabetes, immunity and infection, it causes the degradation of lymphocyte activation and a decrease in macrophage activity in ketosis and hyperglycemia and in case of diabetes complications, it is more severe.19 Like in HIV positive patients, HIV reduces T-lymphocyte activity.20 Even in blood tumor patients, there is a problem in cell-mediated immune response. Alcohol abuse increases the severity and number of infections, ethanol abuse inhibits glottis closure, and alcoholic hepatocirrhosis and ascites cause bacteremia.16 Chronic renal failure is the cause of serious infection in association with decreased cell-mediated immunity and phagocytosis.21 Lastly, old age contributes to non-maturing T lymphocytes, an increase in autoantibody formation and a higher incidence of monoclonal gammopathy.22 With aging, there are many changes in the immune system and cell division and a lot of decreased function of stem cells increase the susceptibility to pathogen infection, which appears in several clinical forms such as increase of cancer prevalence. Aging affects on both cell-mediated and humoral immune responses, and among them, T-cell ability is most related to the immune deficiency in the elderly.23 In such elders, severe dehydration requiring hospitalization occurs more frequently due to acute diarrhea and complications are common. This also increases mortality because of the association with decreased immunity, hypoacidity, decreased bowel movement, malnutrition and other underlying chronic diseases.3
In several studies to date, although the risk of acute diarrhea is high in immunocompromised hosts including the elderly, and acute diarrhea has clinical significance including extension of hospitalization period and increase of mortality,14 most studies have been conducted on infants, children, healthy adults and the elderly based on the results of sentinel surveillance projects so far.178
From January 2013 to July 2014, we conducted diarrhea virus, bacteria and Clostridium difficile toxin tests in immonucompromised patients, including those aged 65 and over, who were admitted to the hospital due to acute diarrhea in the Busan area. The incidence of diarrhea by clinical symptoms and each cause and its related complications and mortality were investigated in order to provide information on the diagnosis, treatment and prevention of acute diarrhea in immunocompromised patients.
MATERIALS AND METHODS
1. Subjects
The prospective study was conducted with 73 patients (30 outpatients and 43 emergency room patients) who were admitted to one tertiary hospital due to acute diarrhea disease from January 2013 to July 2014.
The acute diarrhea symptoms were defined as diarrhea started within 14 days with more than 3 times a day and at least 200 g of feces.
The functional diarrheas due to bacterial infection, parasite or protozoa diseases and irritable bowel syndrome were excluded.
Immunocompromised hosts were defined as adults aged 18 and over with HIV infection, solid tumor, blood tumor, leukopenia with less than 1000/µL, using immunosuppressant (anti-cancer drugs, immunosuppressant, and taking dosage corresponding to 15 mg of prednisolon a day for more than 2 weeks), transplant patients, chronic diseases (diabetic, alcohol abuse, chronic hepatic disease, chronic renal disease, dialysis, and chronic heart failure) and adults aged 65-and over.
2. Study Methods
To study the characteristics of subjects, the patients' age, sex, chronic disease (diabetes, alcohol abuse, chronic hepatic disease, chronic renal disease, dialysis, and chronic heart failure), HIV infection, solid tumor, blood tumor, leukopenia, use of immonosuppressant, transplant patients and treatment history of patients were investigated.
In order to study the clinical characteristics, diarrhea pattern, vital signs (blood pressure, pulse rate, breathing rate and temperature), possibility of food poisoning, related digestive system symptoms, history of antibiotics use within one month, initial blood tests and presence of white blood cells in the feces were investigated. For prognosis evaluation, the hospitalization, use of antibiotics, naturally treated or not and death status were studied. To assess the cause of acute diarrhea, diarrhea virus using feces samples, bacterial culture test, C difficile toxin test and parasite egg test were conducted. The basic salmonella spp. and shigella spp. tests were performed and tests for Campylobacter bacteria, Vibrio bacteria, Bacillus cereus bacteria, and Clostridium perfringens bacteria were performed if suspected.
This study was conducted with the approval of Institutional Review Board of Kosin University Gospel Hospital (Approval No. 13-036).
3. Test Methods
1) Virus Tests
1)-1. Sample pretreatment and RNA extraction
1 g of fecal specimen was added to 9 mL of phosphate buffered saline, shaking by adding 3 to 4 glass beads. The suspended specimen was taken and centrifuged at 4 ℃ for 20 minutes at 3,000 rpm (UNION 32R PLUS®, Hanil, Korea) and the supernatant was used in this study. RNA extraction from each specimen and cell culture medium was conducted in the Te-MagS (Tecan®, Switzerland) which is the extraction device by using the viral nucleic acid extraction kit.
2) Bacteria test
C. difficile toxin test was carried out using Xpert C. difficile assay (Xpert CD assay®, Cepheid, USA). And, salmonella spp. and shigella spp. culture test were incubated at 35 to 37 ℃ for 24 ± 2 hours by inoculating in an SS agar medium and MacConkey agar medium and the colony was confirmed.
4. Statistical Processing
Among 73 patients who were admitted due to the acute diarrhea, the analysis for clinical symptoms and treatment results was conducted for 55 immunocompromised hosts who corresponded to the inclusion criteria by comparing the C. difficile patient group and the non-patient group. SPSS version 22.0 (SPSS Inc., Chicago, IL, USA) was used to compare the two groups using t-test if the dependent variable was a continuous variable, and using chi square test if the dependent variable was a categorical variable. The significance was expressed as the P-value and if it is less than 0.05, it was determined as statistically significant.
RESULT
1. Characteristics of subjects
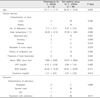
From January 2013 to July 2014, among 73 patients who were admitted to the hospital due to acute diarrhea, the subjects were 55 immunocompromised hosts including 19 males (34.5%) and 36 females (65.5%) who didn't fit the inclusion criteria of acute infectious diarrhea (Table 1).
The immunocompromised hosts used in the study included 36 patients aged 65 and older (65.5%), 17 diabetes patients (30.9%), 2 chronic hepatic disease and alcohol abuse patients (3.6%), 17 chronic heart disease patients (30.9%), 7 chronic renal disease patients (12.7%), 14 dialysis patients (25.5%), 8 solid organ transplant patients (15.1%), 15 solid tumor patients (27.3%), 3 blood cancer patients (5.5%), 7 leukopenia patients (12.7%), 5 patients taking immunosuppressant (9.1%), 8 patients taking steroids (14.5%), and 2 patients with gastrointestinal structure abnormality (3.6%) (Table 1).
There were 8 patients with no underlying diseases (14.5%), 16 patients with one type of disease (29.1%), 19 patients with two diseases (34.5%), 12 patients with three diseases (21.8%) and 33 patients among 36 patients aged 65 and over had more than one disease (Table 1).
2. Clinical Features and Treatment Results
Among the patients analyzed, there were 6 cases (10.9%) of suspected food poisoning and 10 cases (18.2%) of unidentified causes (Table 2).
There were 22 cases (40%) that had a history of using antibiotics before 1 month and 33 cases (60%) of not using antibiotics (Table 2).
The type of diarrhea was mostly watery for 35 patients (63.6%) and loose stool for 20 patients (36.4%) and the number of feces was mostly less than 3 times a day (Table 2).
The accompanied symptoms were abdominal pain for 18 patients (32.7%), nausea for 14 patients (26.4%), vomiting for 6 patients (11.3%), and decreased urine volume for 4 patients (7.5%) (Table 2).
When looking at the form of hospitalization, 44 patients (80%) were admitted in the general ward, 9 patients (16.4%) were in the intensive care unit and only 2 patients (3.6%) were visited as outpatients. Also, 22 patients were hospitalized through outpatient and 33 patients were through emergency room. 14 patients (25.5%) recovered using a conservative treatment and 41 patients (74.5%) were treated with antibiotic administration. There were no deaths or recurrence (Table 2).
3. Analysis of Diarrhea Pathogen
During the study, diarrhea virus, salmonella spp., shigella spp. and parasite eggs were not detected in patient samples. 6 patients (10.9%) were positive in C. difficile toxin test (Table 3).
4. Comparison of C. difficile patient group and non-patient group
As a result of comparing C. difficile patient group and non-patient group detected in this study, the temperature was 36.4 ± 0.1 ℃ for patient group and 37.1 ± 0.8 ℃ for non-patients group, and the serum creatinine was 1.2 ± 0.8 mg/dL for patient group and 2.6 ± 2.5 mg/dL for non-patient group, which showed significant difference (P < 0.05). However, since the fever was not over 38℃ and the patients with chronic renal disease and dialysis were included, it was not clinically significant. In addition, there were no statistically significant difference in age, underlying diseases, clinical characteristics and treatment type (Table 4).
DISCUSSION
The most commonly reported diarrhea virus in the studies to date on the source of infection for acute diarrhea in immunocompromised hosts was Norovirus.9 Clinical features of Norovirus and immunocompromised hosts related to this were known; in the case of admitted patients aged 60 and over due to acute diarrhea, there was a 30 day difference in survival time depending on the presence of other underlying diseases if the pathogen was Norovirus (89.5% vs. 94.7%) and also the matched-control study for patients aged 80 and over showed 30 days of survival difference (81.2% vs 91.4%).24 According to another study by Ignacio A et al., when analyzing the diarrhea samples in patients with solid organ transplant who were admitted due to acute diarrhea, the most common infections were C. difficile, Norovirus and cytomegarovirus.25
In this study, there was a detectable difference between diarrhea virus and bacteria. 6 cases of C. difficile toxin detection were the only identified causative pathogen.
When considering the reason why no other bacteria or viruses were detected besides C. difficile in this study compared with other studies to date, the reason would be as follows: first, enteric pathogens other than C. difficile had a detection rate of 3.3 to 10% at 3 days before hospitalization, while after 3 days it is reduced to 0 to 0.7%.2627 In this study, the diarrhea samples were collected from immunocompromised hosts who were hospitalized due to acute diarrhea as a main complaint. However, there were patients whose collection were not completed at 3 days before the hospitalization due to the difference of hospitalization method, and in samples 3 days after the hospitalization, the possibility of bacteria other than C. difficile to be cultured became very low. Second, the number of subjects included in this study was small (55 patients) and may have affected the results of pathogen detection. In addition, due to the pricing issues, tests for other pathogens such as cytomgalovirus could not be performed in addition to tests for virus (Norovirus, astrovirus, sapovirus, rotavirus, and adenovirus), C. difficile, Salmonella spp., shigella spp. and parasite eggs. Also, when looking at the characteristics of past studies on diarrhea virus during the hospitalization period of most nursing facilities or hospitals, there were more reports on diarrhea that were spread via an epidemic than by sporadic occurrence. However, in this study period, there was no epidemic diarrhea virus in the hospital or community, so it can be thought that the detection rate of diarrhea virus was low.28 In this study, several limitations that prevented pathogens other than C. difficile to be detected should be considered, but considering the general increase of the elderly population, the increase in the number of immunocompromised hosts including the elderly admitted to nursing facilities, and the high proportion of elderly patients in the diarrhea patient group, it is necessary to perform the tests for C. difficile among other tests for pathogens of acute diarrhea based on the results of this study.
In this study, from a total of 55 subjects, 41 subjects (74.5%) received antibiotic treatment for acute diarrhea, which mostly was empirical administration based on clinical judgment. There were 2 cases treated through outpatient visit, and most cases were hospitalized. Among these cases, 9 subjects (16.4%) were in severe state, requiring admittance to the intensive care unit. It is known that most infectious diarrhea patients just need the conservative treatment to recover by visiting outpatient or emergency room. On the other hand, in this study there were many cases of severe symptoms requiring hospitalization during the initial occurrence in the treatment of immunocompromised hosts and there was more frequent use of empirical antibiotics as the treatment for diarrhea. As a result of treatment, all patients recovered and there were no deaths. When looking at studies on the empirical use of antibiotics in acute diarrhea in immunocompromised hosts, there were cases requiring antibiotic treatment due to the clinical severity and the possibility of complications but the immunocompromised hosts referred in these cases were the patient group corresponding to the criteria of immunocompromised hosts suggested in this study.29 Empirical antibiotic use in the treatment of acute diarrhea has benefits and limitations; as for benefits, it is necessary for fast relief of diarrhea symptoms, suppression of disease progression, and relieving symptoms such as fever, abdominal pain and vomiting, and as for limitations, these include the occurrence of side effects, emergence of resistant strains, increased costs, and increased risks of complications in shiga toxin secreting E. coli infections.30 In this study, it is difficult to state clearly due to the limitations such as lack of immunocompromised hosts and the difference in the immunocompromised degree, however, it is necessary to consider the appropriate antibiotic use, considering that acute diarrhea in immunocompromised hosts shows more severe conditions than diarrhea in other patients or people in the community who do not have acute diarrhea. Additionally, it is necessary to have enough studies on acute diarrhea in immunocompromised hosts distinguished from healthy people by complementing the limitations of this study. The clinical characteristics and prognosis were compared by dividing the study group into patients with and without detectable C. difficile, however, this didn't show any significant difference due to the small number of subjects. Complementing these problems in further studies will be a good idea. There were limitations to discover and conclude the infectious etiology of acute diarrhea in immunocompromised hosts epidemiologically only with this study, however, considering the existing published researches mentioned earlier that the incidence of CDAD increased, it is necessary to consider CDAD in the future sentinel surveillance project with immunocompromised hosts including the elderly.
It can be considered that the limitation of this study was the difference in the degree of immune depression depending on the difference in underlying diseases between subjects, and among them the immune suppressed patients who have reduced T-lymphocyte function was included in the broad sense. For example, of 36 patients aged 65 and over, there were 11 patients with more than 3 underlying diseases, 13 patients with 2 underlying diseases, and 9 patients with 1 underlying disease. There were differences in the types and number of underlying diseases but the entire subject group exhibited compromised T lymphocyte function compared to general public. Therefore, analyzing this study considering these facts can be the basis for further studies. In addition, analyzing the difference in the pathogenic degree, clinical characteristics and pathogens in acute diarrheas of the immunocompromised hosts and general public under the same condition will be helpful in many ways.
In conclusion, patients recover from most diarrheas naturally, so it is not necessarily to apply a bacterial identification test or antibiotic treatment. However, acute diarrhea occurring in immunocompromised hosts who are the subject of this study could have severe symptoms or prognosis. Therefore, pathogen detection may have an important impact on the treatment and prognosis of patients and in some cases, the consideration of empirical antibiotic use is necessary. In this study, other virus or bacteria besides C. difficile were not detected, however, if further studies are performed by complementing the limitations of this study, politically useful results may be obtained. Additionally, based on the results of this study, it is necessary to consider testing for the C. difficile strain through the sentinel surveillance project for community health care.



 XML Download
XML Download