

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Parathyroid carcinoma is very rare in patients with primary hyperparathyroidism, only accounts for 1% to 2% of all cases. It is characterized by higher incidence of renal dysfunction, metabolic bone disease and gastrointestinal symptoms. Although the clinical manifestations of hyperparathyroidism are more severe in patients with parathyroid carcinoma when compared to those with those with parathyroid adenoma, it is difficult to differentiate carcinoma from adenoma without pathologic confirmation. To our knowledge, there have only been a few cases of hyperparathyroidism due to parathyroid carcinomas reported to date. Here, we report a case of 63-year-old woman developing osteoporosis, hypercalcemia and hypophosphatemia due to a parathyroid tumor and was diagnosed with parathyroid carcinoma postoperatively.
Figures and Tables
 | Fig. 1Bone mineral density of L-spine and left femur neck shows osteoporosis of L-spine and left femur neck. (BMD, bone mineral density)
|
 | Fig. 2Thyroid sonography shows extrathyroidal solid mass at right lobe with containing cystic portion (2.2 × 4.6 × 1.6 cm); (A) Transverse view, (B) longitudinal view.
|
 | Fig. 3Parathyroid scan with 99mTc-sestamibi scan shows irregular parathyroid mass below right thyroid gland with high uptake after two hours delayed image. (ANT, adenine nucleotide translocator)
|
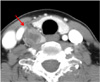 | Fig. 4Neck computed tomography demonstrates non-enhanced parathyroid mass (2.7 × 2.0 cm sized) below the posterior portion of right thyroid gland that has extended to the inferior portion of thoracic inlet and marginal irregularity. There is no lymph node enlargement.
|
 | Fig. 5Microscopic feature of parathyroid mass reveals a rather well circumscribed but partially infiltrating tumor tissue which consists of uniform, polygonal clear cells with mild nuclear pleomorphism. A few foci of vascular invasion and capsular penetration are noted (hematoxylin and eosin staining); (A) × 40, (B) × 400.
|
References
1. Mittendorf EA, McHenry CR. Parathyroid carcinoma. J Surg Oncol. 2005. 89:136–142.

2. Busaidy NL, Jimenez C, Habra MA, et al. Parathyroid carcinoma: a 22-year experience. Head Neck. 2004. 26:716–726.
3. Shane E. Clinical review 122: Parathyroid carcinoma. J Clin Endocrinol Metab. 2001. 86:485–493.
4. Bates D, Clark NG, Cook RI, et al. American College of Endocrinology and American Association of Clinical Endocrinologists position statement on patient safety and medical system errors in diabetes and endocrinology. Endocr Pract. 2005. 11:197–202.
5. DeLellis RA. Parathyroid carcinoma: an overview. Adv Anat Pathol. 2005. 12:53–61.
6. Mazzaglia PJ, Berber E, Kovach A, Milas M, Esselstyn C, Siperstein AE. The changing presentation of hyperparathyroidism over 3 decades. Arch Surg. 2008. 143:260–266.
7. Potts JT. Fauci AS, Braunwald E, Kasper DL, editors. Diseases of the parathyroid gland and other hyper- and hypocalcemic disorders. Harrison's principles of internal medicine. 2008. 17th ed. New York: Mc Graw-Hill.
8. Kim JK, Koh YB. A case of parathyroid carcinoma. J Korean Surg Soc. 2002. 62:173–177.
9. Levin KE, Galante M, Clark OH. Parathyroid carcinoma versus parathyroid adenoma in patients with profound hypercalcemia. Surgery. 1987. 101:649–660.
10. Edelson GW, Kleerekoper M. Hypercalcemic crisis. Med Clin North Am. 1995. 79:79–92.
11. Ariyan CE, Sosa JA. Assessment and management of patients with abnormal calcium. Crit Care Med. 2004. 32:S146–S154.
12. Clark OH, Okerlund MD, Moss AA, et al. Localization studies in patients with persistent or recurrent hyperparathyroidism. Surgery. 1985. 98:1083–1094.
13. Stark DD, Gooding GA, Moss AA, Clark OH, Ovenfors CO. Parathyroid imaging: comparison of high-resolution CT and high-resolution sonography. AJR Am J Roentgenol. 1983. 141:633–638.
14. Koea JB, Shaw JH. Parathyroid cancer: biology and management. Surg Oncol. 1999. 8:155–165.
15. Hundahl SA, Fleming ID, Fremgen AM, Menck HR. Two hundred eighty-six cases of parathyroid carcinoma treated in the U.S. between 1985-1995: a National Cancer Data Base Report. The American College of Surgeons Commission on Cancer and the American Cancer Society. Cancer. 1999. 86:538–544.
 XML Download
XML Download