

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Osteoporotic fractures of the pelvic ring are not uncommon, and sacral insufficiency fractures (SIFs) are often overlooked in patients with buttock or low back pain following no or minimal trauma, which results in diagnostic delays.1
SIFs are often bilateral and commonly associated with other fractures, most frequently a pubic ramus fracture.2-4 However, it remains unclear which fracture (sacral or pubic rami) occurs first, and in cases of bilateral SIFs, whether fractures occur simultaneously or sequentially. Only one English report has described this sequence, and in this report it was suggested initial disruption is likely to occur in the sacrum, and that the subsequent instability creates mechanical failure of the pubic rami.5
We encountered a patient with sequential bilateral SIFs that occurred after one side superior and inferior pubic rami fractures. To our knowledge, this is the first case to show a clear sequence of pelvic insufficiency fracture. We describe this case and include a relevant review of the literature. The patient provided informed consent that case data could be submitted for publication.
CASE REPORT
A 74-year old woman was referred from a local hospital to our institute to rule out the possibility of a metastatic bone tumor in the right sacrum. She complained of right buttock pain of 2 weeks duration. She had a history of slip down 3 months previously and right superior and inferior pubic rami fractures were diagnosed at a local hospital based on simple radiography and computed tomography (CT) findings (Fig. 1). She has been admitted at the local hospital and been treated conservatively (oral medication and tolerable ambulation after 4 weeks bed rest). After a month of conservative treatment, she was able to walk without pain. She had no previous history of radiation therapy, corticosteroid usage, or inflammatory disease.
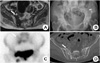
Before presentation at our institute, she had revisited the same local hospital for right buttock pain and had undergone pelvic magnetic resonance imaging (MRI) (Fig. 2A). The radiologist involved decided to rule-out the possibility of a metastatic tumor, and thus, she was referred to our hospital.
At presentation, she underwent X-ray, CT, and a bone scan. In pelvic anteroposterior (AP) view, callus formations were observed on the right superior and inferior pubic rami and increased radiopacity in the right sacrum (Fig. 2B). On the Tc-99m hydroxymethane diphosphonate (HDP) bone scan, hot uptake was present in the right superior and inferior rami and right sacrum (Fig. 2C). CT showed a fracture line in the right sacral alar, which was confirmed by a radiology specialist as SIFs (Fig. 2D). We also evaluated her bone marrow density, and found severe osteoporosis at the lumbar spine (average T score for L1-4 = -3.3). She was then admitted and rested for 4 weeks on oral analgesia. After 1 week of rest, the pain subsided to the extent that she was able to tolerate walking with a walking aid. After 4 weeks, she was allowed tolerable weight-bearing ambulation and discharged.
However, one month after discharge, she re-presented our outpatient clinic complaining of left buttock pain of duration 1 week. CT was re-performed and a new fracture line was observed at the left sacral alar (Fig. 3A). On this occasion, she was also managed conservatively, as described above. Weight bearing ambulation was allowed 4 weeks later and osteoporosis medication was continued. At the time of writing (12 months after re-presentation), the buttock pain was completely resolved (Fig. 3B).
DISCUSSION
SIFs were first reported in 1982,6 but the incidence of SIF remains unknown. Nevertheless, its potential prevalence within the general population was highlighted by Weber et al.4 after a 2-year prospective study. In this study, it was found that the frequency of SIF in women aged over 55 years who presented to hospital with low back pain was 1.8%.
The subject of the present study was referred to our hospital to evaluate the possibility of a sacral bone tumor, and we might easily have arrived at this diagnosis based on pelvic CT and Tc-99m bone scan findings. Schindler et al.7 said CT was the most reliable imaging technique for the diagnosis of SIFs, because Tc-99m bone scanning was highly sensitive but non-specific and MRI of the fractures may mimic metastatic disease.
Furthermore, it is known that the associated fractures are present in 25 to 80% of patients with SIFs.2,4,7 Pubic rami fractures are most common, followed by vertebral compression fractures, iliac wing fractures, and intertrochanteric hip fractures. Plain radiography combined with technetium bone scanning is most sufficient at detecting these associated fractures.2,5,7 De Smet and Neff5 concluded SIF may precede pubic fractures by 3~4 months, and that the latter follows a protracted healing course as compared with the former. Other authors have similarly reported high frequencies of concomitant pubic fractures in variable proportions.2,4 Pelvic biomechanics dictates that disruption of the bony skeleton at one site may increases stresses in other regions of the pelvic ring. De Smet and Neff5 suggested that initial disruption is likely to occur in the sacrum and that the instability created results in mechanical failure of the pubic rami. Accordingly, they advised that the detection of a pubic rami fracture should raise clinical suspicion of a coexistent SIF in high risk patients with senile osteoporosis.
However, in our case, fractures of one side of the pubic rami developed earlier than the SIF, which may have been because our patient had experienced a slip down. Nevertheless, 3 months after she sustained the right superior and inferior rami fractures, a right SIF occurred, and this was followed 2 months later by a left SIF. We believe that in the described case severe osteoporosis was the fundamental cause of all pelvic fractures, and that biomechanical disruption of the bony skeleton at the anterior pelvis and walking stress increased stresses at the ipsilateral sacrum and then at the contralateral sacrum.
Linstrom et al.8 reported insufficiency fractures caused by cyclic loading of osteoporotoic bone, and ambulation was the activity that had the distribution of stress within the sacrum. They also described walking model that displayed maximal stress at characteristic location for pelvic insufficiency fracture, included acetabular region, pubic and ischial rami, and inner curve of the iliac wing. So sequential SIFs may occur not only after fracture of rami like present case, but also fracture in other site of pevic ring, if patient did not restrict ambulation after injuries of pelvic ring.
The majority of SIFs are treated conservatively. Medications including calcium and vitamin D, bisphosphonates, and calcitonin and all should be continued to reduce the risk of further insufficiency fractures.9 Recently interventional treatment methods, such as, sacroplasty and percutaneous screw fixation have been reported,10 but these methods are only available in a limited number of specialized centers. Furthermore, evidence supporting their widespread use over conservative management is lacking.
Our patient was treated conservatively with bed rest and oral analgesia followed by gradual mobilization with walking aids as pain allowed at 4 weeks. In our patient, after each SIF, pain was relieved by about one week of bed rest, and thus, we did not consider surgical management.
Although severe osteoporosis is the fundamental cause of SIF, we suggest that SIFs can occur after pelvic ring injury in any side because biomechanical disruption of the pelvic ring can increase stress on sacrum. Thus, even after conservative treatment of a pelvic insufficiency fracture (a rami fracture or a sacral fracture) if the patient complains of pain in the pelvic area, we advise that the presence of another insufficiency fracture be considered.


 XML Download
XML Download