

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In general, maxillary canines contain only single root and root canals, therefore, only few recent studies regarding maxillary canines with two root canals have been reported.1,2 This case report will demonstrate a maxillary canine is composed with two root canals which are completely separated, therefore, it will generate more precise understanding of anatomical variations of the maxillary canine.
CASE REPORT
A 58-year-old man was referred to Luden dental clinic. The main complaint of the patient was severe and continuous pain on the left side of maxillary canine. The tooth was over-prepared because it would be the abutment tooth of a removable partial denture. Any unusual medical histories were not revealed. The clinical examination revealed a pin point pulp exposure in the tooth, and the severe pain was found while the ethyl chloride temperature test and the percussion test were performed. Preoperative radiographic findings were revealed no specific periapical pathosis (Figure 1).
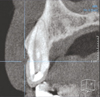
On the basis of clinical findings, an irreversible pulpitis of the tooth was diagnosed and endodontic treatment was planned. During the first visit, the access cavity was opened under local anesthesia with 2% lidocaine. Only one root canal orifice was found on the labial side after access cavity opening. The working length was measured with an electronic apex locator (Root ZX, Morita, Tokyo, Japan) and the pulp was extirpated completely using a K-hand file (Kerr, Romulus, MI, USA). At the second visit, the pain was partially relieved, however a positive response to the percussion test was revealed. A cone beam computed tomograph (CT) scan (Implagraphy SC, Vatech, Yongin, Korea) was taken with a 1 mm-thick section. The sagittal plane image of the cone beam CT scan revealed the presence of an additional curved canal on the palatal side (Figure 2). The palatal canal orifice was identified by extending the access cavity to the palatal side (Figure 3). After the working length of the palatal canal was measured using the electronic apex locator, a periapical radiograph was taken (Figure 4). The periapical radiograph revealed two separated root canals. Using a rotary nickel-titanium file (ProFile, Dentsply Maillefer, Ballaigues, Switzerland), the root canals were shaped to #40 by the crown-down method.
At the third visit, remaining discomfort disappeared completely, and the root canals were filled with gutta-percha (Diadent, Chongju, Korea) and root canal sealer (AH Plus, Dentsply Maillefer, Konstanz, Germany) (Figure 5). The patient did not have any specific symptoms or abnormalities during the 6-month follow-up period.
DISCUSSION
When the anatomical anomaly is observed in the radiographic findings at the first examination, corresponding abnormalities on the opposite side must be suspected. In this case, the radiographic image of the opposite canine of the patient showed a Vertucci Type II (2-1) (Figure 6). Although there are limitations in radiographic image and possibilities of incomplete endodontic treatment, the results also showed a bilateral anatomical anomaly in this case. In this regard, they had stated "The more rare the aberration, the more likely it is to be bilateral in occurrence".1
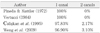
Generally, it is considered that all maxillary canines only have a single canal.2,3 However, two studies have been reported that a maxillary canine is composed with two root canals in the possibility of the ranges of approximately 2 - 3% as the below Table 1.4,5 These studies related to the root canal anatomy of the maxillary canine are summarized in Table 1.
In summary, the root canal system of the maxillary canine seems to be diverse. However, this facts were hard to be demonstrated due to difficulties in identifying the various anatomy in the root canal system since roentgenographic or simple staining methods were used. In the other hand, new methods are now being used, including micro CT6 and cleared teeth technique2 to allow three-dimensional identification of the complex aspects of the root canal system. The root canal systems of all teeth including the maxillary canine possible to be demonstrated to be relatively complicated patterns.
There has been only one case report that showed the presence of maxillary canine which has one root and two root canals.7 However, the reported canine is a type II (2-1) according to the Vertucci classification in which the separated root canals converge with each other at the apex. In this case; however, the maxillary canine has two separate orifices and root canals that communicate at the middle third of the root. According to the Vertucci classification, the present case can be classified as type VI (2-1-2) which has not been reported yet. This case has been provided a broader understanding of anatomical variations in the maxillary canine.
CONCLUSIONS
Lots of anatomical variations exist in the root canal system8 and the maxillary canine has been found of containing with two root canals. If both root canals have not been appropriately treated during endodontic treatment, the necrotic tissue may remain after the treatment, and it may negatively affect prognosis. 9 For example, if only one side of root canals has been treated, the severe pain might be revealed. Therefore, to treat complete removal of any infection and prevention of re-infection, the clinician should be well aware of the possibility of anatomical variations in the root canal system.





 XML Download
XML Download