

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Since calcium hydroxide has been introduced to endodontics by Hermann in 1920, it has been used widely in many endodontic applications in dentistry.1 The most common uses of calcium hydroxide in dentisty are an inter-appointment intracanal medication during root canal treatment and pulp capping agent because of its high pH, antimicrobial effect and hard tissue stimulation.2-4 Due to these properties, calcium hydroxide is also used for the following applications; apexification of immature teeth, inhibitor of inflammatory root resorption, and healing of large periapical radiolucent lesions. In these cases, calcium hydroxide may be used for months to years until the desired effects are accomplished. For apexification, the longer periods are required for immature teeth to stimulate the formation of an apical hard tissue barrier before completing the root canal filling with gutta percha. However many previous reports have been reported that long-term application of calcium hydroxide in root canal may weaken the root dentin and result in the tooth fracture. Cvek reported that incidence of cervical root fracture is relatively high in endodontically treated immature teeth either spontaneously or due to minor impacts.5 Andreasen et al. measured the fracture strength of immature mandibular incisors from sheep for 0.5, 1, 2, 3, 6, 9, or 12 months and the results showed markedly decrease in fracture strength with increasing storage time for calcium hydroxide dressing group, indicating that the fracture strength of calcium hydroxide-filled immature teeth will be halved in about a year due to the root filling.6 Rosenberg et al. measured the effect of calcium hydroxide root filling on the microtensile fracture strength (MTFS) of 40 extracted human permanent maxillary incisors and reported a weakening of the dentin by 23% between 0 days (control) and 84 days and 43.9% between 7 and 84 days.7 These findings may be of importance in the decision of treatment plans for teeth with pulp necrosis and immature root formation. The results of these studies confirmed the view that long-term exposure of root dentin to calcium hydroxide may affect its physical properties.
Dentinal strength might, in part, depend on the link between its two main components, hydroxyapatite and collagenous networks.6,7 Part of the organic matrix is composed of acid proteins and proteoglycans containing phosphate and carboxylate groups. These substances may act as bonding agents between the collagen network and the hydroxyapatite crystals. Calcium hydroxide may, due to its strong alkaline nature, neutralize, dissolve, or denature the carboxylate and phosphate groups leading to a collapse in the dentin structure.
In infected mature teeth with apical periodontitis, however, the common treatment is put calcium hydroxide in the root canal for short periods of time, 1 or 4 weeks. Thus it is important to know the short-term effects of calcium hydroxide on the root dentin strength in human mature teeth. The strength of the teeth can be measured using the fracture strength test. The purpose of this study is to determine whether short-term application of calcium hydroxide in the root canal system for 1 and 4 weeks affects the fracture strength of human permanent teeth. The null hypothesis is that it can reduce the fracture strength of human permanent teeth with increasing storage time.
MATERIALS AND METHODS
Sample preparation
This study used 32 mature human single rooted mandibular premolars in similar size and dentin thickness without decay or restorations, which had been extracted in orthodontic clinic. Radiographics were taken in both mesiodistal and buccolingual views to measure the size and dentin thickness. An endodontic access cavity was prepared in each tooth using a high speed hand piece and a No. 4 round bur. And then working length was measured by protruding a file until the tip of a file could be visualized beyond the apical foramen and subtracting 0.5 mm from this measurement.8 The root canals were instrumented to a size 20 K file to the working length and mechanically prepared using ProTaper NiTi rotary instruments (Dentsply Maillefer, Ballaigues, Switzerland) at 300 rpm. All canals were enlarged from a size S1 to F2. Irrigation between each filing with 0.5 mL of 5.25% NaOCl. Then the teeth were assigned to two groups randomly, control and experimental group, and subdivided into 1 week test and 4 weeks test group with 8 teeth in each group.
Tooth samples of group 2 were dried with paper points, and then packed with calcium hydroxide paste (Calcipex II, Nippon Shika Yakuhin Co., Shimonoseki, Japan) and sealed coronally with caviton (Caviton, GC Co., Tokyo, Japan) to imitate the endodontic procedure. To guarantee tight contact with the canal walls and a compact packing of the canal space, excess Ca(OH)2 was deliberately squeezed out the apical foramen.9 The canal of group 1 tooth samples were left empty. The apicies of all the samples were sealed with acrylic resin, submerged in normal saline and put in a storage box at 37℃ to mimic the oral environment. After 1 and 4 weeks, samples were removed from the storage box for fracture strength test.
Fracture strength test
Each tooth was submerged in acrylic resin cylinder block to the cemento-enamel junction. The fracture strength was measured using a universal testing machine (Instron Series IX, Instron Corp., Canton, MA, USA). The samples were fixed into a vice and the load was applied at the cement-enamel junction at 90° angle to long axis of the tooth at 5 mm/min by cross-head speed (Figure 1). The maximum load required to fracture the samples was recorded and data were analysed statistically by the two way ANOVA test at 5% significance level.
RESULTS
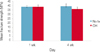
The mean fracture strengths of two groups after 1 week and 4 weeks were similar. There was no statistically significant difference between experimental groups and between time intervals. After 4 weeks, the mean fracture strength of calcium hydroxide treatment groups reduced approximately by 8.2% compared to no treatment groups: an average of 39.23 MPa for no treatment and 36.01 MPa for CH group. However, there was no statistically significant difference (p > 0.05, Figure 2). Most of fracture was happened in cervical root area (Figure 3).
DISCUSSION
This study investigated whether short-term application of calcium hydroxide in the root canal system for 1 and 4 weeks affects the fracture strength of human permanent teeth. The results showed that the calcium hydroxide placed in the root canal for 4 weeks weakened the strength of the root dentin approximately by 8.2% compared to the control group (no treatment). Though the results of this study confirm the results of the previous studies, the decrease rate of the fracture strength is not as much as the results of the previous studies. Rosenberg et al. reported weakening of dentin by 23% after 28 days in human permanent maxillary incisors.7 White et al. investigated the bovine teeth for 5 weeks maintained in petri dishes and found that calcium hydroxide could decrease the fracture strength by 32%.10 Sahebi et al. also evaluated the effects of short-term calcium hydroxide application on the strength of human permanent dentin against the compressive forces with 50 extracted mature human mandibular single rooted permanent premolars and found that teeth subjected to 30 days application of calcium hydroxide required less compressive force to break root dentin cylinders.11
Anderssen and Hasselgren et al. reported a dissolving effect when calcium hydroxide contacts pulp tissue for just 1 week.12,13 There is few information about the fracture strength of endodontically treated human teeth. And calcium hydroxide is used widely for immature tooth for apexification for a long term to initiate an apical hard tissue which has been found to occur after 9 - 18 months.14,15 Many previous reports found that long term use of calcium hydroxide in the root canal may weaken roots and result in the fracture failure of immature teeth. But there is few report of fracture strength changes of human teeth in response to endodontic materials. This is one of a few studies to examine whether short-term application of calcium hydroxide in the root canal system for 1 and 4 weeks affects the fracture strength of human permanent teeth. In this study, after 4 weeks, the mean fracture strength of calcium hydroxide treatment groups reduced approximately by 8.2% compared to no treatment groups. However, there was no statistically significant difference.
However, there are a few limitations in this study. The major limitation of this study is that the method could not reproduce clinical situations. In the present study, each tooth was embedded in acrylic resin cylinder block to the cemento-enamel junction. Research studies have found that the Periodontal ligament (PDL) plays an important role in the mechanisms for tooth trauma. And it is well known that the PDL act as shock absorbers to minimize external impact. Rees reported that PDL is an important structure for distribution of stresses generated by load application to the teeth.16 Also Soares et al. reported that the root embedding method and the type of PDL simulation can affect the fracture modes and when roots were embedded in a rigid structure without simulating the PDL, the fracture patterns tended to occur at the limit of the resin cylinder.17
In this study, force applied to cervical area of tooth vertically at a constant rate until it is fractured. In a clinical situation, any force that may cause a tooth fracture is likely to be a sudden impact force rather than a continuously applied force. And clinically, force is likely to be applied at varying angles to the tooth structure rather than being vertical to cervical area. Additionally, test result could be affected by examiner's inaccuracy in embedding the teeth to CEJ junction and in making acrylic resin block with same powder/liquid mixing rate.
In conclusion, these result suggest that short term calcium hydroxide application is available during endodontic treatment. Further research will be required using the method applicable to clinical situations with PDL simulation, forces applied in a different manner and a different direction and with minimum examiner's error.


 XML Download
XML Download