

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Patients with recently exposed root surfaces may become susceptible to acidic environments, even when other pertinent environmental factors remain unchanged.1 The inorganic chemical events of the root caries are similar to that of the enamel, however, the permeability and reactivity of the root surface allows the demineralization process to occur at a higher pH than in enamel.2 Therefore, clinicians observe that many patients may appear resistant to enamel caries but prone to root caries, after root surfaces become exposed by soft tissue recession, traumatic tooth brushing habits, periodontal treatment, and etc. For exposed root surfaces, fluoride varnish has been advocated both by serving as a desensitizing agent and an anticariogenic agent.3 Fluor Protector (1,000 ppm F, Ivoclar Vivadent, Schaan, Lichtenstein), 0.1% silane fluoride containing varnish is known not only to supplement additional fluoride ions but also to block a porous structure by building a polymerized barrier.4 Several studies have demonstrated the prolonged caries inhibition effect of Fluor Protector, even though it has a low fluoride concentration (1,000 ppm F) relative to other varnishes containing 5% NaF (22,600 ppm F, Duraphat, Colgate, New York, NY, USA; Duraflor, Medicom, Tonawanda, NY, USA; CavityShield, 3M ESPE, St Paul, MN, USA).3,5,6 However, it was shown that dentin required higher levels of fluoride to reach a level of inhibition comparable to that of enamel.7,8 Ettinger et al. suggested that the depth of artificial lesions on root surfaces are dose responsive to the concentration of fluoride used, and that 10,000 ppm F was beneficial.9 For root dentin, polymerbased varnishes may penetrate into dentinal tubules and act as a type of sealant. But, Hong et al. evaluated the efficacy of varnish with the consideration of abrasive contact in the daily circumstance and showed that preventive effect of varnish was diminished by tooth brushing.10
Most studies on the efficacy of fluoride varnish have focused on high caries risk groups in clinical situations or induced severe acidic challenges in in vitro experiments. It has been rarely addressed about caries inhibition activity of varnish for a normal population who do not additionally require a preventive intervention. However, a previously low to moderate risk group, who practice regular tooth brushing and preclude any drastic cariogenic challenges, may become newly susceptible to the disease due to their recently exposed root surfaces. And, the fluoride varnish can be applied in a preventive measure, even before any clinical signs of caries development are perceived.
Traditionally, the initial stages of carious lesions are characterized by partial dissolution of the tissue, leaving a 20 - 50 µm thick, rather well-mineralized surface layer and a subsurface body of the lesion with a mineral loss of up to 30 - 50%.11 Such a detectable amount of disintegration is resulted from the preceding continuum of reactive chemical events. To quantify the beneficial effects of fluoride for the initiation of the pathologic change, it may be useful to trace the elemental redistribution with a fine resolution.12 In this study a scanning electron microscope (SEM, JEOL JSM-6610LV, JEOL, Tokyo, Japan) and an energy dispersive spectrometer (EDS, Oxford instruments, Bucks, UK) were employed to measure quantitative changes in mineral composition and to locate the demineralized layer. A confocal laser scanning microscope (CLSM, Zeiss LSM-Pascal, Carl Zeiss, Göttingen, Germany) was used to determine the depth of varnish penetration into root tissue. We hypothesized that low concentration fluoride varnish applied to the root surface would influence the early profile of subsurface demineralization under a mild acid challenge.
MATERIALS AND METHODS
Specimen preparation
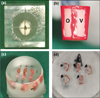
This study was approved by the Institutional Review Board of Seoul National University Dental Hospital. Ten human lower premolars extracted for orthodontic treatment were used within 6 months of extraction and disinfected in 0.5% chloramines-T and stored in distilled water at 4℃. The teeth were inspected to ensure that they were free of fractures or other defects, and the periodontal ligament was removed using a Gracey curette under microscopy. The crowns of the teeth were removed at the cementoenamel junction with a low-speed diamond saw (Isomet, Buehler Ltd., Lake Bluff, IL, USA) and the apical roots were removed leaving 4-mm-long root segments. The segments were sectioned mesiodistally and buccolingually into four parts (Figure 1). Each quarter root was covered with a thin layer of acidresistant nail varnish, creating two 1 mm × 4 mm windows on the outer root surface and randomly assigned into one of four experimental groups (Table 1).
Each group was divided into two subgroups; v (varnish application) or o (no varnish application).
Fluoride varnish application and pH cycling
Fluor Protector (1,000 ppm F) was applied on one of the two windows of each specimen according to the manufacturer's directions and dried for 5 minutes. After storage in 100% humidity for 24 hours at 37℃, the thin varnish layer was pulled off using a No.15 surgical blade. The specimens were immersed in 2 mL of demineralizing solution (1.4 mM Ca, 0.9 mM P, 0.05 M acetate buffer, 0.03 ppm F, pH 5.0) for 3 hours, followed by immersion in 2 mL of remineralizing solution (1.5 mM Ca, 0.9 mM P, 0.1 M Tris buffer, 0.05 ppm F, pH 7.0) for 20 hours.13,14 After 5 days of cycling, specimens were immersed in remineralizing solution for 2 days. Solutions were changed for each immersion and placed in a 37℃ incubator without agitation.
SEM/EDS analysis
Specimens were embedded in epoxy resin (Epofix, Struers, Glasgow, UK) and horizontally cross-sectioned along the midline (Figure 1). The exposed cut surfaces were serially polished with 500, 1,300, and 2,400 grit Al2O3 abrasive papers, followed by 1 and 0.25 µm diamond and 0.1 and 0.05 µm alumina polishing suspensions (Struers, Copenhagen, Denmark). The specimens were ultrasonically cleaned in deionized water for 10 minutes, dried for 72 hours in a desiccator and carbon sputter-coated. On the crosssectioned surfaces, the demineralization bands were identified at ×600 magnifications in a phase contrast of backscattered electron imaging (BSI) mode of SEM. To identify variations in the amounts of elements from the outer surface throughout the inner dentin, two line analyses with a 120-µm span were performed perpendicular to the outer root surface (Figure 2). The spot measurements at 1-µm-pixel intervals were obtained from the observation areas (surface layer, demineralized layer, and sound dentin) which were identified in SEM images. Each measurement within the observation area was summed and averaged into a single value for analysis. The unit of value was the intensity of the characteristic x-ray per 200 msec, which indicated the relative weight of each element. A fluorapatite crystal (3.38% fluoride) was used as a standard for Ca, P, and F. Operating conditions for both the image and elemental analyses of EDS were 15 kV of accelerating voltage and 50 nA of beam current.
CLSM analysis
Six premolars were de-coronated, and the root segments were mesiodistally sectioned into halves. Each buccal segment had a window of 3 mm × 4 mm produced via application of nail varnish. The windows were coated with 0.4 mL of Fluor Protector mixed with 10 ppm by weight of propidium iodide (Calbiochem, San Diego, CA, USA). After storage in 100% humidity for 24 hours at 37℃, the varnish layer was pulled off. The specimens were mounted, sectioned, and polished in the same way as for the SEM/EDS analysis. The polished surfaces were examined with CLSM using a C-Apochromal ×40 water lens with an additional ×40 objective lens and ×2 digital zoom (×800 total magnification). A He/Ne G laser was used with an excitation band at 543 nm wavelength and a 560 nm-long pass filter.
Statistical analysis
The Ca and P contents in the sound dentin were set to 100%, and the loss of the contents in the surface layer and in the demineralized layer were calculated as a % (Table 3, Figure 2). The distribution of caries lesion depth and weight loss of Ca and P in percentages were found to be approximately normally distributed using the Shapiro-Wilk test (p > 0.05). To compare the mean lesion depth between single and double pH cycling groups, the analysis of variance (ANOVA) with the Tukey's multiple comparison method was used. The mean weight percentages of Ca and P between the with and without varnish groups were compared using the paired t-test. Based on the evaluation of the SEM images of the specimens in the Group Ao, five teeth were assigned to the thick-cementum group and five teeth were assigned to the thin-cementum group. The mean weight percentages of Ca and P between thick- and thin-cement groups were evaluated using an independent t-test. A p value of 0.05 was selected as the threshold for statistical significance. Analyses were performed using SPSS version 12.0 statistical software (SPSS Inc., Chicago, IL, USA).
RESULTS
SEM exhibited demineralization band formation underneath root surfaces that had undergone pH cycling (groups B, C and D), while such demineralization was not observed in group A (Figure 2). The average lesion depth (SD) in the single pH cycling groups (groups B and C) was 12.5 (2.5) µm, significantly smaller than the average lesion depth in the double pH cycling group (group D), 19.4 (3.8) µm (p < 0.05, Table 2). There were no significant differences in lesion depths between subgroups o (no varnish) and v (varnish) within each group (p < 0.05).
In group A, no changes in the Ca and P contents from the outer surface to the inner dentin depth of 120 µm were distinguishable, and the loss was set to 0%. In the surface layer, between the varnish and no varnish groups (Ao/Av, Bo/Bv, Co/Cv and Do/Dv), there were no significant differences in Ca content (p < 0.05). But, Bv and Cv had significantly higher P loss, as compared with each counterpart (Bo and Co) (p < 0.05). In the demineralized layer, the Ca and P contents significantly decreased in all groups except group A (p < 0.05). These patterns of elemental change were concordant with the microscopic images (Figure 2). The average Ca loss (SD) was 13.4 (4.8)% in the single pH cycling groups (groups B and C) and 12.7 (7.1)% in the double pH cycling group (group D). The average P loss (SD) was 17.5 (11.1)% in the single pH cycling group and 13.0 (7.0) % in the double pH cycling group. There were no significant differences in Ca and P loss between the single pH cycling and the double pH cycling groups (p < 0.05). Between the varnish and no varnish groups, Ca and P loss were significantly higher in Cv than in Co in the demineralized layer (p < 0.05).
The mean thickness (SD) of cementum was 38.4 (18.8) µm in the thick-cementum group and 2.8 (4.4) µm in the thin-cementum group. There were no significant differences in lesion depth or in Ca and P contents between the thick-cementum group and the thin-cementum group (p < 0.05) (Table now shown). The teeth from the thick-cementum group had a demineralized layer within the cementum layer (Figure 3). An image of the varnish applied to the root surface is shown in Figure 4. Varnish impregnation into the root surface is represented by the red fluorescent band. The depth of impregnation did not exceed 15 µm in any specimen.
DISCUSSION
In this study, we induced a low level of pH cycling on root surfaces and evaluated the influence of fluoride varnish on the initiation of root caries. Among the three experimental groups that were subjected to pH cycling (groups B, C, and D), in group B, pH cycling initiated demineralization and varnish was used as a potential therapeutic agent. Group C represented clinical situations in which varnish is applied to sound root surfaces as a preventive measure, and then the varnish-coated surface was subjected to an acid challenge. In group D, an initial lesion was created on the root surface, and varnish was applied. The tooth was then subjected to a second pH cycling to determine how the varnish-treated lesion would react to a persistent acid challenge. We applied pH cycling without agitation and produced a purely intact surface layer width of 10 - 15 µm and a demineralized subsurface layer with less than 20% mineral loss. Our second pH cycling extended the lesion, increasing the depth of both the surface layer and the demineralized layer. The surface layer remained well-mineralized, implying that the original minerals in the surface layer acted like a nucleus of mineral growth and an ion transport barrier.15 In the subsurface layer, multiple electrodense bands appeared in the SEM images, demonstrating the dynamic process of mineral loss and gain. This observation scope was relatively small, considering the resolution of conventional microradiography and light microscopy used in previous studies.10,14 In this study, SEM was shown to be useful in detecting minute changes in initial caries development. Also, it may be applicable to elaborate a dose-response relationship of non-operative caries control protocols in future studies.
Quantitative analysis of the mineral composition of the root substrate is influenced by individual variation. 16 We split a single tooth into quarters, allocating the pieces equally into four groups, to minimize substrate differences. The window to which the varnish was applied was compared to the adjacent non-varnish window in order to decrease location variance. The baseline Ca and P contents were set at the inner dentin, where the Ca and P levels plateaued in scan analysis. Using these values, we determined the volume percentages of demineralization in reference to a standard value acquired from sound dentin, as other studies did in microradiographic analysis.17 Our single cycling (5 days pH cycling plus 2 days remineralization) without agitation induced no significant loss of Ca or P in the surface layer, but a mild amount of demineralization in the subsurface layer. The second cycle only increased the total width of the reactive zone, i.e. in both the surface layer and the subsurface demineralized layer. And Ca and P contents were at levels similar to those following the first cycling. We were interested in determining how fluoride would affect the surface-preserved demineralized lesion. On mineral-dissolved enamel and dentin, fluoride promotes the formation of fluoridated hydroxyapatite. However, a well-preserved surface layer may block ion transport to the deeper lesion, and the fluoride-driven remineralization process may not occur as readily as in lesions with a mineral-deficient surface layer.15 In our study, no additional remineralizing patterns were demonstrated in the varnish subgroups of all three experimental groups. In other way, it was shown that varnish application dissolved more P from the surface layer in groups B and C and more Ca and P from the demineralized layer in group C (p < 0.05). Acidulated fluoride solutions dissolve enamel slightly and deposit substantial amounts of calcium fluoride on the tooth surface.18 Similarly, the acidic Fluor Protector (pH 2.5, measured in our study) reacts with dentin which has half the mineral content of enamel.19 The erosive changes from the acidic nature seemed to be recovered by further pH cycling. The levels of Ca and P were regained by the second cycling, and the Dv group did not show a significant difference from the Do group (p < 0.05). SEM demonstrated the unique profiles of cementum and dentin, although their elemental distribution did not differ (Figure 3). Since cementum naturally has the same mineral distribution as dentin, its demineralization pattern may not be different.2,20 Our analysis supported the claim that cemental caries underwent a change in elemental composition similar to that of dentin caries.
We intentionally removed the varnish layer to create mechanical wearing that occurs after a certain period of time in an oral environment, and to simulate the appropriately brushed root surfaces of a low risk population. The peeled-off varnish layer may still be effective if the varnish had penetrated into porosities and remained as impregnated remnants. Fluor Protector has a thin consistency and good wetting effect on both dry and hydrated dentin substrates.21 However, using CLSM, Arends et al. showed that retention of Fluor Protector was limited to the outer surface, which is similar to other varnish products.21 They applied the varnish on the surfacesoftened lesions and produced a barrier with a thickness of 10 µm, which was consistent with our observations of the surface-preserved lesions. We attempted to detect any increased levels of fluoride in the surface zone, but were unable to do so, likely due to the low content level. Most studies using Fluor Protector employed a relatively severe acid challenge, resulting in some amount of surface disintegration, which may be more relevant to a high caries risk population.3,5,6 In a high risk situation, the physical presence of the varnish enhances the redistribution of ions in the body of the caries lesion by creating a favorable gradient for inward fluoride diffusion and reduces the porosity of the lesion.4 Under less severe conditions, the surface layer is well preserved, and an additional varnish barrier may not be advantageous. Silane, a bifunctional coupling agent with hydrophilic functional groups, is not stable in a hydrous environment.22 A silane-based varnish may be as permeable as other polymerizable dentin adhesives and may provide an ion passage into the subsurface area. Our results were in accordance with those of a previous study that demonstrated that sound dentin with Fluor Protector applied was affected equally by pH cycling, relative to dentin without varnish.23
Recently, the use of not only fluoride varnish but also fluoride containing dentin adhesives and desensitizing agents have been advocated to protect root dentin from caries formation. The submicron level elemental analyses may be applicable to the quantification of anticarious activities afforded by physical protection of a film barrier and by the chemicotherapeutic effect of fluoride ions. Within the limits of this in vitro study, silane-based fluoride varnish did not affect demineralization patterns produced under a mild acid challenge. Varnish was restricted to the intact surface layer and did not penetrate into the subsurface area where mineral loss occurred.






 XML Download
XML Download