

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
As a result of concerns that arose nearly 40 years ago, efforts were made to standardize endodontic files and root canal filling materials. This resulted in an international standard for endodontic files, known in the United States as ANSI standard No. 58 and No. 28. The taper of the instruments is prescribed to be 0.02 taper of length, starting at the tip. Three standard lengths are available as 21 mm, 25 mm, and 31 mm. The working part of the instrument must be at least 16 mm.
After introduction of nickel-titanium (Ni-Ti) to endodontics since 1988, Ni-Ti hand files and rotary instruments have become popularized because of their properties of superelasticity and shape memory.1 Ni-Ti files also have standard length (21 mm, 25 mm) except several orifice shapers.2-5
For the size of the rubber stop is 1 mm, it is possible to perform canal shaping up to 20 mm, based on endodontic working length, when using 21 mm file. However using a long length file is uncomfortable since these Ni-Ti files should be mounted on a handpiece and can't apply precurvature. In clinical procedure of endodontic treatment, the time for patients to keep their mouth open is longer than in any other treatment. If the time of mouth opening increases, patient will feel discomfort and side-effects like temporo-mandibular joint disease might occur.6,7 Using long instruments will also give difficulties during the treatment procedures for the operator too.
The lengths of the endodontic instruments are designed to be based on the length of the tooth. There are several methods for measuring these lengths of the teeth.8 There are methods like, measuring directly from extracted tooth, surveying from the radiographic films or by measuring the working length of the tooth.9 This method of measuring working length of the tooth can be done by measuring the length of the extracted tooth, using radiographic references or by using electronic working length measuring instruments. In vivo study, the radiographs are not always reliable because they can show considerable deviations depending upon the angles of the X-ray cone.10 The apical constriction of the the root also does not coincide with the anatomic apex.8,11,12 It is deviated linguo-buccally or mesio-distally from the root. If the exit deviates bucco-lingually, it is very difficult to locate accurately the position of the apical foramen using only roentgenograms, even with multi-directed angles.13
The electric apex locator (EAL) machine has attracted a great deal of attention because it operates on the basis of the electrical impedance rather than by a visual inspection.13 EALs help to reduce the treatment time and the radiation dose, which may be higher with conventional radiographic measurements. In addition, EALs were reported to be an accurate14-18 and reproducible method as the newest third generation type and can acknowledge a root perforation.
International standard follow the average tooth lengths of caucasian people.9,19,20 Although there were reports on the average tooth length of caucasian people, few information on the differences of canal lengths between the races is available.
Therefore, the aim of this study was to investigate average working lengths of Korean posterior teeth and evaluate validity of endodontic file length.
Materials and Methods
Six hundred and seventy Korean patients who received a root canal treatment of posterior teeth at ○○ University between 2006 and 2008 were randomly selected and classified with data warehouse (Sybase IQ 12.6, Sybase, Oakwood, US). Teeth with severe dental caries, fixed prosthesis, or those that were impossible to negotiate the apical region due to calcification or other reasons were excluded. 2nd mesio-buccal canal of maxillary molar and mandibular molar with C-shaped canal were excluded.
The clinical procedures for the root canal treatment were executed by single operator. Access cavities were made using the standard clinical procedures and 0.5 mm occlusal reduction from marginal ridge was performed. The endodontic working lengths were first measured using an electronic measuring device (Root-ZX; J. Morita Co., Kyoto, Japan), and the lengths were then verified by taking periapical radiographs. Any electronic length within 1.0 mm of the radiographic tooth length was regarded as a reliable initial working length.11 Only the initial working length was used in this study because the working length might change as the canal became enlarged.21
These measured endodontic working lengths were record on computer based charts then abstracted and conversed by ETCL program (Data Stage 7.1, IBM, New York, US) which then stored at data warehouse. Data from measured endodontic working lengths were analyzed by OLAP program (Hyperion Intelligence 8.5, Oracle, Redwood, US).
Endodontic working lengths of 487 premolar canals and 870 molar canals were measured in this study. Mean and standard deviation of endodontic working length of the each tooth were computed than frequency distribution classified by length was measured. Normal distribution classified by length using mean and standard deviation was measured.
Results
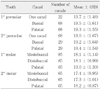
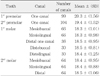
The endodontic working lengths of posterior teeth in Korean are given in Table 1 and 2. It is showing the number of surveyed canals per canal location, mean value and standard deviation for each tooth. Maxillary premolar was classified into subclasses according to the number of canal, premolars with 1 canal and premolars with 2 canals. Identically mandibular 1st molar were classified according to the number of the distal canal, into molars with 1 distal canal or molars with 2 distal canals.
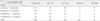
Table 3 shows the number of canal per each length of molars. Total of 487 canals of molar were measured and maxillary first premolar with less than 20 mm of endodontic working length were counted up to 112 whereas calculated up to 324 canals when all 4 premolar were considered. Canals of premolar which was less than 22 mm by length was summed up to 465.
Table 4 shows the number of tooth per each length of premolars. Total of 870 canals of premolar were measured and maxillary first molar with less than 18 mm of endodontic working length were counted up to 149 whereas calculated up to 549 canals when all 4 molar were considered. Canals of molar which was less than 20 mm by length was summed up to 831.
Figure 1 shows the normal distribution and frequency distribution sorted by the length of the premolar, the mean value (19.54 mm) and standard deviation (1.62) of the premolars. The right side of the vertical axis shows the number of frequency which 19 mm was most frequent, numbering 66, followed by 18 mm, 20 mm and 20.5 mm in sequence according to the frequency deviation. The scale at left side of the vertical axis shows the probability of normal distribution. Figure 2 shows the normal distribution and frequency distribution sorted by the length of the molar, the mean value (18.21 mm) and standard deviation (1.10) of the molars. Scale at right side of vertical axis shows the number of frequency as same as Figure 1. Taking look at the frequency deviation, 18 mm was most frequent, followed by 19 mm, 17 mm in sequence according to the frequency deviation.
Discussion
This study was performed to find out the properness of length of the standard endodontic files for the endodontic working length of Korean, by examining the endodontic working length of premolars and molars of Korean. As mentioned at the introduction, for the size of the rubber stop is 1mm, it is possible to perform canal shaping up to 20 mm, based on endodontic working length, when using 21 mm file. In the case of the premolar, 66.5% of the working length was under 20 mm, and 95.4% were under 22 mm. According to the fact that the standard endodontic files on the market is usually 21 and 25 mm, 21 mm file is not sufficient to use for premolar and for that reason the length of the files must be at least 23 mm for adequate use. For the case of the molar, 86.9% of the working length was under 19 mm and 95.5% were under 20 mm. Considering the endodontic working length, files shorter than 20 mm is not suitable for the molar and it must be longer than 21 mm for adequate use.
Various studies are conducted to improve the intraoral accessibility of the instruments of endodontic treatment. For the case of Ni-Ti file, development of micro hand piece instead of existing contra-angle low speed hand piece made it much easier to apply into the patient's oral cavity. For some files, K3 rotary Ni-Ti file (SybronEndo, Orange, Califomia, US) for example, handle design were shortened without affecting the working part of the instrument to develop the intra-oral accessibility.5 Consequently, choosing the proper length of the instrument for the patient's working length will affect the intra-oral accessibility.
At most of the files the rubber stop has the thickness of approximately 1.0 mm. This is thought to be because the rubber stop must have some rigidity during the filing process. However if the rubber stop can be made thinner with certain rigidity, the length of the instruments can be shorter to that extent.
Occlusal reduction was performed for every endodontic treatment of the posterior teeth in this study. Occlusal reduction was carried out to set a fixed reference point during the measurement of endodontic working length. Occlusal reduction was set 0.5 mm lower form the marginal ridge to minimize the error of reduction amount of each tooth. It could have been set based on the cusp, but variations according to the amount of abrasion might be severe, so marginal ridge were set to be the basis.
Crown restoration has to be carried out to reinforce the weakened tooth during the endodontic treatment. For tooth preparation for the crown restoration, 1.5 mm at the occlusal surface must be reduced. Considering this fact, occlusal reduction during the endodontic treatment of posterior tooth can be carried out up to 1.5 mm for the max. 21 mm file was the most proper length of the file for posterior tooth as the result of this study, however if the thickness of the rubber stop can be reduced and the amount of occlusal reduction is controlled, shorter files might be able to be used for the canal shaping.
The length of the teeth is already being measured by various methods in several studies.22-26 The data acquired from extracted tooth or method using radiographic pictures can be useful for studies on anatomical form, size and length, but it is not useful to decide the length of the instruments of endodontic treatment in actual clinical use.
In this study, the endodontic working lengths were measured instead of the length of the tooth. This is because the endodontic instruments (ex: file, GGD bur) is used on clinical practice based on the endodontic working length. There are reports that previous study also measured the endodontic working length, but was limited into a portion of teeth, which is different with this study.27
There is body of opinion that there are difference in root canal lengths between Asians and western population with the latter having longer teeth. Kim et al. researched the difference of the tooth length of Korean and Occidentals and reported that there is difference between those two. In this study, the endodontic working length of the Korean was measured to inquire most adequate file length.
Various programs were used in this study in order to abstract and analyze the data (computer based charts, ETCL program, data warehouse, OLAP program). This method will ease the effort to find the data recorded separately, and will be utility to use in framing all kinds of dental statistics later on.
Conclusions
The aim of this study was to investigate average working lengths of Korean posterior teeth and evaluate validity of endodontic file length. In this study, the endodontic working length of the posterior teeth of 670 Korean patients were measured than each mean value and standard deviation were investigated than the frequency deviation and standard deviation per each length were calculated. As the result, following conclusion was acquired.
Among the canals of premolar, 66.5% of canal length was marked under 20 mm by endodontic working length and 95.4% could be measured under 22 mm.
With the result of measurement of endodontic working length of premolars of Korean, it suggested that 23 mm endodontic file is more proper than the 21 mm and 25 mm file on the market.
Among the canals of molars, 95.5% of canal length was marked under 20 mm endodontic working length.
With the result of measurement of endodontic working length of premolars of Korean, it suggested that 21 mm endodontic file on the market can be used for most canals.
The most proper length of the instruments for majority of the canal shaping was found in this study by measuring the endodontic working length of Korean. Adequate length of the instrument will be useful both for the patients and the operators.



 XML Download
XML Download