

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
The development of adhesive dentistry has allowed that the crown fragment reattachment can be another option in the treatment of crown fracture. However, additional crown lengthening procedure or extrusion of the tooth may be necessary in the treatment of crown root fracture because subgingival fracture line in close proximity to the alveolar bone leads to challenges for restorative procedure and the violation of the biologic width. This case report presents a modified crown fragment reattachment technique of crown root fracture with pulp exposure, which was done without additional crown lengthening procedures. After the endodontic treatment, the patient was treated using a post insertion and the fragment reattachment technique, which made it possible to preserve the space for the biologic width and maintain a dry surgical field for adequate adhesion through the modification of the fractured coronal fragment. Since a coronal fracture was occurred and reattached afterward, it was observed that the coronal fragment was well maintained without the additional loss of periodontal attachment through 2-year follow up.
Figures and Tables

Figure 2
Removed fragment of the fractured tooth. Fracture line was located 3 mm under CEJ. CEJ, cementoenamel junction.
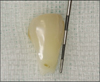
Figure 3
Papilla preservation flap was reflected for crown reattachment procedure. Fracture line was extended to the equigingival area.

Figure 4
Adaptation of the modified fragment using premade putty index. Margin of the coronal fragment was trimmed off and it is short from the bone margin.

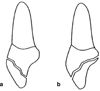
Figure 5
Rubber dam was placed with #211 clamp and fiber post was inserted (a). Coronal fragment was cemented with Duolink (b).

Figure 6
Fracture line was covered by composite resin with external chamfer preparation due to strengthening the cemented fragment.





References
1. Andreasen FM, Noren JG, Andreasen JO, Engelhardtsen S, Lindh-Stromberg U. Long-term survival of fragment bonding in the treatment of fractured crowns: a multicenter clinical study. Quintessence Int. 1995. 26:669–681.
2. Farik B, Munksgaard EC, Kreiborg S, Andreasen JO. Adhesive bonding of fragmented anterior teeth. Endod Dent Traumatol. 1998. 14:119–123.

3. Reis A, Loguercio AD, Kraul A, Matson E. Reattachment of fractured teeth: a review of literature regarding techniques and materials. Oper Dent. 2004. 29:226–233.
4. Andreasen JO, Andreasen FM, Andersson L. Textbook and color atlas of traumatic injuries to the teeth. 2007. 4th ed. Copenhagen, Denmark: Munksgaard;314–336.
5. Reis A, Francci C, Loguercio AD, Carrilho MR, Rodriques Filho LE. Re-attachment of anterior fractured teeth: Fracture strength using different techniques. Oper Dent. 2001. 26:287–294.
6. Loguercio AD, Mengarda J, Amaral R, Kraul A, Reis A. Effect of fractured or sectioned fragments on the fracture strength of different reattachment techniques. Oper Dent. 2004. 29:295–300.
7. Pusman E, Cehreli ZC, Altay N, Unver B, Saracbasi O, Ozgun G. Fracture resistance of tooth fragment reattachment: effects of different preparation techniques and adhesive materials. Dent Traumatol. 2010. 26:9–15.
8. Grossmann Y, Araúz-Dutari J, Chogle SM, Blatz MB, Sadan A. A conservative approach for the management of a crown-root fracture. Quintessence Int. 2006. 37:753–759.
9. Ertugrul F, Eden E, Ilgenli T. Multidiciplinary treatment of complicated subgingivally fractured permanent central incisors: two case reports. Dent Traumatol. 2008. 24:e61–e66.
10. Padbury A Jr, Eber R, Wang HL. Interactions between the gingiva and the margin of restorations. J Clin Periodontol. 2003. 30:379–385.
11. Eichelsbacher F, Denner W, Klaiber B, Schlagenhauf U. Periodontal status of teeth with crown-root fractures: results two years after adhesive fragment reattachment. J Clin Periodontol. 2009. 36:905–911.
12. Olsburgh S, Jacoby T, Krejci I. Crown fractures in the permanent dentition: pulpal and restorative considerations. Dent Traumatol. 2002. 18:103–115.
13. Frantz BJ, Polson AM. Tissue interactions with dentin specimens after demineralization using tetracycline. J Periodontol. 1988. 59:714–721.
14. Lowenguth RA, Polson AM, Caton JG. Oriented cell and fiber attachment systems in vivo. J Periodontol. 1993. 64:330–342.
15. Dean JA, Avery DR, Swartz ML. Attachment of anterior tooth fragments. Pediatr Dent. 1986. 8:139–143.
16. Stellini E, Stomaci D, Stomaci M, Petrone N, Favero L. Fracture strength of tooth fragment reattachments with postpone bevel and overcontour reconstruction. Dent Traumatol. 2008. 24:283–288.
 XML Download
XML Download