

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
Successful root canal treatment requires an understanding of root canal morphology and anatomy. Accurate diagnosis of root canal morphology and anatomy is essential for thorough shaping and cleaning of the entire root canal system and consequent successful root canal treatment.1) Mandibular premolars show a wide variety of root canal anatomy.2) There seems to be a racial predisposition for the presence of two or more canals in maxillary and mandibular premolars, as well as their bilateral occurrence.2,3) Especially, the occurrence of three canals with three separate foramina in mandibular premolars is very rare. Vertucci4) and Zillich et al5) reported the occurrence of three canals in mandibular first premolars at 0.5% and 0.4% respectively. Their studies in second premolars showed these percentages at 0.0% and 0.4%, respectively. To our knowledge, however, there is rare case report about treatment of mandibular second premolar with three separate canals divided at the apical level of the root whereas most previous reports showed that the orifices were found in the mid root section.6) The present case report describes the root canal treatment of a mandibular second premolar having three independent root canals with separate foramina.
II. Case Report
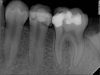
A 27-year-old man with a noncontributory medical history was referred because of occasionally slight spontaneous pain in the mandibular left second premolar. The tooth was diagnosed as irreversible pulpitis and initiated to have root canal treatment by general dentist 2 days ago, but could not negotiate all of the root canals. After this treatment, the initial acute symptom had been relieved, but the tooth was still symptomatic and tender to percussion. A radiographic image of the tooth showed an unusual anatomy of these teeth (Figure 1). According to clinical and radiographic examination, a diagnosis of pulp necrosis with apical periodontitis was made.
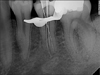
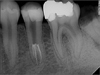
The tooth was anaesthetized, isolated with rubber dam and temporary filling was removed. The apical third was explored to locate the canal orifices using the operating microscope (OPMI Pico Dental Microscope; Carl Zeiss, Oberkochen, Germany). Three separated root canal orifices were found on the same level of the pulp chamber floor at a depth of 14.0 mm: one lingual, one distobuccal, and one mesiobuccal. Each canal had separate portal of exit. The working lengths of root canals were determined using an electronic apex locator (Root ZX; J Morita Inc., Kyoto, Japan) and then verified by a radiograph (Figure 2). The working lengths of three canals were same as 19.0 mm. In addition, endodontic ultrasonic tips (CPR tips; Spartan, Fenton, MO, USA) were used to achieve better straight-line access. Small, slightly pre-curved K-files were used to debride the canals and to establish a glide path to the working length. The canals were cleaned and shaped using nickel titanium rotary instrument (Protaper Universal; Dentsply-Mailiefer, Ballaigues, Switzerland). After drying the canals with paper points, all canals were obturated with warm gutta-percha technique with AH 26 (Dentsply, Konstanz, Germany) root canal sealer (Figure 3). A post-operative radiograph showed separate three root canals (Figure 4).
III. Discussion
In this case, the mandibular second premolar with three root canals could be treated successfully using a non-surgical method. The possibility of variations in root canal morphology must be considered before root canal treatment is undertaken.7) Careful interpretation of the root outline and the periodontal ligament space may suggest the presence of an extra root or canal.8) During the initial placement of scouting files in the assumptive site as canal orifice, clinicians may encounter an obstruction and the files may deflect to the buccal, lingual, mesial or distal before it travels any further. This may indicate a canal division. Therefore, it is important to develop a sense of tactile feeling and direction with appropriate precurved scouting files to detect the multiple canal orifices.
When working under the microscope, clinicians can see the sodium hypochlorite bubbling in the extra canal, marking its presence. Furthermore, once it has been established that there are three canals, it is important to obtain straight-line access to all canals. This may be achieved by ultrasonic tips, which reduce stress on the files used subsequently to shape the canals and minimize the risk of instrument separation and canal transportation.
In this case, tooth had the C-shaped canal shape as category II9) of the mesiobuccal and ligual distinct canal. Extravagant use of small files and sodium hypochlorite is a key to thorough debridement of narrow canal isthmus. Despite the existence of complicated dental anatomy, shaping outcomes with nickel-titanium rotary files prepares the canals to a predetermined shape. Furthermore, warm gutta-percha filling technique has shown to allow the creation of excellent adaptation of filling material to root canals.

 XML Download
XML Download