

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
Most of the teeth that require endodontic treatment have lost more tooth structure than just an access preparation1). After endodontic therapy, considerable loss of dentin including anatomic structures such as cuspal ridges and the arched roof of the pulpal chamber was observed. Many dentists assume that endodontically treated teeth are weakened and more prone to be fractured due to desiccation or premature loss of fluids supplied by vital pulps2), and access preparations result in greater cuspal flexure, increasing the probability of cuspal fracture3).
If endodontic access can be conservative and proximal tooth structure remains intact, simple restoration of the endodontic access opening may be adequate. Lewinstein and Grajower4) found that endodontic treatment did not affect the Vickers hardness number of human cervical root dentin. Fusayama and Maeda5) demonstrated that there were no changes in the modulus of elasticity, hardness, or fracture toughness of pulpless teeth.
Composite resin is the most popular core material. Pilo et al.6) showed that composite cores have fracture resistance comparable to amalgam and cast post and cores. Restoration using composite resin provided substantial recovery of tooth stiffness, especially when coupled with etching of dentin7).
When immediate restoration of tooth after completion of root canal treatment is not possible, the root-canal system should be protected by sealing the canals and floor of the pulp chamber with intracoronal barriers8). This increase in strength occurs equally well if the composite resin is placed as a reinforcing base or as the sole restoration9). Glass ionomer cement (GIC) increased the resistance of the cusps to fracture when used as a base but surprisingly not when used as the sole restoration10).
Noncarious cervical lesions, characterized by the loss of dental hard tissue at the cementoenamel junction (CEJ) in the absence of caries, are conditions commonly encountered in dental practice11). More recently, an additional mechanism for cervical tooth loss that links with occlusal loading has been proposed12). Clinically, abfraction lesions are sharp, angular, wedge-shaped lesions that sometimes have a subgingival location and often associated with marked wear facets13). And according to Telles et al.14), the most commonly affected teeth are the maxillary premolars.
The main problem for endodontically treated posterior teeth is the depth of the cavity15). Even breaking the continuity of the enamel by cutting a class I cavity may reduce the tooth rigidity16). The presence of an occlusal restoration increased cuspal movement which in turn increased the shear forces around the buccal class V cavity, and this effect was more marked for increases in depth of the occlusal preparation17).
There are many studies1,18-20) concerning intracoronal mesioocclusodistal (MOD) restoration of endodontically treated maxillary premolars. But, it is hard to find the study which deals with the restoration of endodontically treated maxillary premolars with notch-shaped class V cavity.
Finite element analysis (FEA) is a sophisticated computer modeling technique that was introduced in the early 1960s in the aircraft industry. FEA is a mathematical method in which the geometry of a specimen is divided into a sequence of distinct elements interconnected at nodes. Physical and mechanical properties of the specimen are assigned to each element and the loading conditions and restraints are applied. It is particularly useful in dentistry since it can readily cope with both the complex geometry of a tooth and it's supporting structures and with the large variation in the physical properties of the tooth, periodontal ligament and alveolar bone21).
The purpose of this study was to evaluate the possibility of success of bonded intracoronal composite resin restoration with or without GIC base of endodontically treated maxillary second premolars with notch-shaped class V cavity using 3D FEA.
II. Materials and Methods
1. Finite element model
To develop a 3D FE model, intact normal extracted human maxillary second premolars were used. The extracted premolars were scanned serially with Micro-CT (SkyScan1072; SkyScan, Aartselaar, Belgium) to expose the tooth sections perpendicular to the long axis of the tooth (58 µm in thickness) and parallel to the occlusal plane. Image processing software, 3D-DOCTOR (Able Software Co., Lexington, MA, USA), was employed to make the boundaries of enamel, dentin and pulp and to construct a surface model of tooth from the sectioned two dimensional images. ANSYS (Swanson Analysis Systems, Inc., Houston, USA) was used to mesh and analyze 3D FE model.
The final model consisted of 27704 elements with 29503 nodes. The physical properties of the tooth and supporting structures used in this study are given in Table 1. All the vital tissues were presumed linearly elastic, homogeneous and isotropic. The corresponding elastic properties such as Young's modulus and Poisson's ratio were determined according to literature survey22,23).
The periodontal ligament was assumed to be 0.3 mm wide, and the dimensions of surrounding compact and cancellous bone were derived from standard texts24,25). The alveolar bone was also generated by growing the outer surface of the tooth model from 2 mm below the CEJ.
In these models, the outer surface of the alveolar bone model was fixed in order to prevent rigid body motion for FEA.
2. Experimental conditions
1). Restorative procedure
Notch-shaped class V cavity and access cavity were filled with hybrid composite resin with or without GIC base. GIC bases were filled up to ideal cavity depth from canal orifice. Four case of simulated model were shown in Figure 1.
The data of material properties such as elastic modulus, Poisson's ratio used in this study were obtained by literature review26,27) (Table 2). The Z100 (3M Dental Products, St. Paul, MN, USA) was used as representatives of hybrid composite resin and Fuji II LC (GC Co., Tokyo, Japan) as GIC base. The conjunctions between materials were set as complete coupling.
2). Loading conditions
As in Figure 2, perpendicular point load of 500 N was applied on the upper third of the lingual incline of the buccal cusp (Load 1) and on the upper third of the buccal incline of the palatal cusp (Load 2).
III. Results
Maximum principal stress analysis under Load 1
1) Buccal surface stress analysis
(1) Pattern of stress distribution
The maximum principal stress distribution along the occlusal cavosurface margin of mid-buccal of N group was broader than S group. Stress concentration was slightly decreased when restored with GIC base (Figure 3).
(2) Analysis of stress
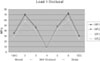
Analysis of stress along the CEJ
Tensile stresses were shown at the node 2 and 8, and in S group, slightly higher tensile stress about 6 MPa was observed than in N group. Compressive stresses were observed along the other area of CEJ. GIC base had no influence on the stress distribution (Figure 4).
2) Occlusal surface stress analysis
(1) Pattern of stress distribution
Extremely high tensile stresses were concentrated around the loading point and moderate high tensile stress along the central groove except access cavity area restored with composite resin. Patterns of stress distribution were similar regardless of experimental conditions (Figure 5).
(2) Analysis of stress
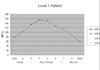
Analysis of stress along the central groove
Peak tensile stress distributions were observed at the marginal ridge area. Lowest tensile stress of 25.35 MPa (SR1) and highest tensile stress of 73.25 MPa (NR2) were observed at the peak, and tensile stresses were slightly higher in N group. There was no difference between the restorations with and without base (Figure 6).
3) Palatal surface stress analysis
(1) Pattern of stress distribution
Slightly more elongated pattern of high stress distribution along the CEJ was observed in N group. There was no difference between the restorations with and without base (Figure 7).
(2) Analysis of stress
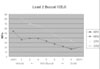
Analysis of stress along the CEJ
High tensile stresses of from 55 MPa (SR2) to 154 MPa (NR1) were concentrated along the CEJ and peak stress of 154.13 MPa was detected on the portion of slight distal to the mid-palatal CEJ. Tensile stresses were slightly higher in N group than S group. There was no difference between the restorations with and without base (Figure 8).
Maximum principal stress analysis under Load 2
1) Buccal surface stress analysis
(1) Pattern of stress distribution
As a whole, the maximum principal stress distributions were different between N and S groups at the CEJ. In S groups, slightly higher tensile stresses than N groups were observed and the stresses of mesial side were higher than distal. There was no difference between the restorations with and without base (Figure 9).
(2) Analysis of stress
Analysis of stress along the CEJ
As a whole, higher tensile stresses were shown in S group than in N group. In S group, peak tensile stress of 82.10 MPa (SR1) was observed at node 2. On the other hand, peak tensile stress of 54.21 MPa (NR1) was observed at the mesial point angle in N group (Figure 10).
2) Occlusal surface stress analysis
(1) Pattern of stress distribution
Overall, the pattern of the maximum principal stress distribution was similar in all experimental simulations. Excessive tensile stresses were concentrated around the loading point and along the central groove except access cavity area restored with composite resin (Figure 11).
(2) Analysis of stress
Analysis of stress along the central groove
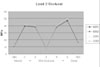
At the areas between margin of access cavity and marginal ridge, peak tensile stress was observed. The values of peak tensile stress were 43.1 MPa (SR2) and 51.3 MPa (SR2) at the node 2 and 6 respectively. Magnitude of stress at the distal point angle was slightly higher than mesial point angle (Figure 12).
3) Palatal surface stress analysis
(1) Pattern of stress distribution
Distribution of tensile stress was not detected along the CEJ. There was no difference in the pattern of stress distribution between the four experimental groups (Figure 13).
(2) Analysis of stress
Analysis of stress along the CEJ
In the distal point angle area of palatal CEJ, slightly high tensile stress of 1 MPa (NR1) was observed. But other areas showed compressive stresses except mesial point angle area. There was no difference in the pattern of stress distribution between the four experimental groups except distal point area (Figure 14).
IV. Discussion
Endodontic therapy causes a pronounced weakening of the tooth and a consequent high risk of cusp or crown fracture. The main problem is that the cusp deflection in an endodontically treated posterior tooth under a given occlusal loading, is markedly greater compared with a vital tooth. The study of Oliveira et al.28) shows that the greatest factor contributing to strength of the endodontically treated premolars is the remaining tooth structure. Especially loss of marginal ridges and the roof of the pulpal chamber as a result of access preparation for the endodontic therapy, may account for the relatively high fracture incidence associated with these teeth29).
However, Reeh et al.1) suggested that endodontic procedures have only a small effect on the tooth, reducing the relative stiffness by 5%. This numerical value was less than that of an occlusal cavity preparation (20%). If access cavity is conservative and both marginal ridges are intact, intracoronal bonded restorations of endodontically treated maxillary premolar can be possible.
Direct composite resin fillings were able to restore the prepared teeth almost to their baseline strength, irrespective of base material30). Trope et al.31) showed that the resistance to fracture of endodontically treated premolars was significantly increased when the teeth were restored with composite resin placed intracoronally after acid etching. Also, GIC used as a base under either a resin or an amalgam restoration increased the resistance to fracture of endodontically treated premolars, but to a lesser degree than the use of the acid etch resin technique10).
Presence of an occlusal preparation has influence on the force distribution around a buccal class V restoration21). Gabel32) was the first one to consider the possibility of occlusal forces affecting class V restorations. There are some clinical evidences for the association of abfraction lesions with heavy occlusal loads. Also, the presence of an occlusal restoration increased cuspal movement which in turn increased the shear forces around the buccal class V cavity17). The result may be the formation of a partial or total gap between the restorative resin and the cavity wall, and thereby a diminished capability of the resin restoration to increase the strength of the tooth33). In this study, both in the condition of Load 1 and 2, tensile stresses of buccal surface were lower in N group than S group except in the case of cervical cavosurface margin under Load 1. It seems that the stress was reduced through the restoration of class V cavity. Also, in case of tooth with class V cavity, stress distribution of buccal surface was unfavorable.
The study of Trope et al.9) showed that if the composite resin is placed as a reinforcing base or as the sole restoration, increase in strength occurs equally well. In this study, there was no difference between the restorations with and without base under Load 1 or 2. Hofmann et al.30) also reported that after placement of the final restorations, there was no longer any difference between teeth with different base materials.
According to the study of Panitvisai and Messer3), because of the inability of dentin to absorb tensile forces once it has been separated from the surrounding tooth structure by a cavity preparation that removed the occlusal enamel cross-bracing structures, there is generally an associated dentin fracture under the tension facet cusp. Eventually, vertical fracturing of the enamel may occur in the marginal ridge zone of the peripheral rim.
In this study, high tensile stresses were concentrated around the loading point and along the central groove except restored access cavity area. The tensile stress of N group was slightly higher than that of S group. The tensile stresses were higher under Load 1 than under Load 2. All of the stress values were over the limit of mechanical properties of the tooth.
Lingual cusps demonstrated coronal fracture most frequently in the posterior teeth of all quadrants. In the maxillary premolars, the lingual cusps were fractured slightly more often than buccal cusps. The removal of hard tissue leaves the remaining cusps flexing outward to a greater degree under a given force, as reflected in the higher strain numbers34).
In the stress analysis of the CEJ of buccal and palatal surface, tensile stress of palatal CEJ under Load 1 was higher than tensile stress of buccal CEJ under Load 2. These results revealed a strong association between loading forces of Load 1 and the possibility of failure of enamel and dentin of the mid-palatal cervical area by tensile stress.
From the results of this study and literature review, palatal cusp fracture is anticipated due to high tensile stress concentration along the palatal CEJ and central groove of occlusal surface especially under Load 1. Therefore the optimal restoration of an endodontically treated posterior tooth should be a cuspal overlays or, if necessary, a full crown when the tooth loaded with heavy eccentric occlusal force.
V. Conclusions
The maximum principal stress distributions were similar regardless of base.
When the load was applied on the upper third of the palatal slope of the buccal cusp, excessive high tensile stress was concentrated around the loading point and along the central groove of occlusal surface. The tensile stress values of the tooth with class V cavity were slightly higher than that of the tooth without class V cavity.
When the load was applied on the upper third of the buccal slope of the palatal cusp, excessive high tensile stress was concentrated around the loading point and along the central groove of occlusal surface. The tensile stress values of the tooth without class V cavity were slightly higher than that of the tooth with class V cavity.












 XML Download
XML Download