

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. INTRODUCTION
Diagnostic assessment in patients with orofacial pain may be challenging due to the close proximity between the teeth and other orofacial tissues, and symptoms associated with neurological disorders. Herpes zoster (shingles) is caused by the reactivation of the latent varicella-zoster virus from a chickenpox infection1). Factors associated with recurrence are older age, immunocompromisation, stress, and tumors affecting the brain or spinal cord2,3).
Herpes zoster may affect any sensory ganglia and its cutaneous nerve, including cranial nerves. Among the cranial nerves, the trigeminal nerve is affected by the reactivation of the latent herpes zoster virus the most. The first division of the trigeminal nerve is commonly affected, whereas the second and third divisions are rarely involved4). If the third division of the trigeminal nerve is affected, it may be characterized by pulpitis in the mandibular molars and vesicular skin eruptions in the affected sensory nerve area.
During the prodromal stage of herpes zoster in particular, the only presenting symptoms may be similar to pulpitis; this may be a diagnostic challenge to the clinician who is not familiar with herpes zoster of the trigeminal nerve5). However, to our knowledge, there have been few case reports on herpes zoster infection involving the third branch of the trigeminal nerve and presenting as odontogenic pain. Therefore, the objective of this report is to present a brief review of herpes zoster infection involving the third branch of the trigeminal nerve, along with a treatment modality and diagnostic considerations.
II. CASE REPORT
A 43-year-old man presented with severe pain and a swelling sensation in the right mandibular molar area. He had been experiencing a severe toothache for two days in the right mandibular area. He reported a history of gold inlay restoration on the right mandibular first premolar, first molar and second molar, which were treated a few years ago.
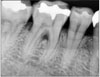
A clinical examination did not reveal a sinus tract or swelling in the patient's face. There were moderate calculus and 4-mm periodontal pockets in the lower molar. No intraoral lesions were observed, and all of the teeth in the lower and upper right quadrant responded normally to cold stimuli, with the exception of the mandibular second premolar, which had little response. Radiographically, no periapical pathosis was apparent (Figure 1 and 2).
Initially, we decided to treat the second premolar due to a tentative diagnosis of apical periodontitis for that tooth. However, no periapical pathosis was seen radographically. Pulpal and periapical diagnostic testing, in conjunction with a radiographic examination, revealed that the second premolar responded normally to all tests, including a percussion test, electrical pulp test, and cold/hot test, and that no periradicular involvement was noted. Furthermore, anesthetic test did not relieve the pain. Therefore it was decided to control the pain with analgesics and to re-evaluate the symptoms in a few days. We also considered the possibility of non-odontogenic pain such as trigeminal neuralgia, migraine, temporomandibular joint disorder, etc.
Three days later, the patient returned to the clinic complaining of intense pain and a rash on the right side of the face. The rash and blisters were localized to the right mandible and chin (Figure 3A). Therefore, we suspected that it might be non-odontogenic pain related to the trigeminal nerve, specifically related to herpes zoster. But it was difficult to accurately diagnose it as herpes zoster. Therefore, we referred the patient to a dermatologist for an accurate diagnosis. The dermatologist reported that it was diagnosed as herpes zoster involving the mandibular branch of the trigeminal nerve. The patient was given antiviral therapy by the dermatologist. It was found that the patient had been given prescriptions for betamethasone, acetaminophen, hydroxyzine, famciclovir, gabapentin, antidepressant, etc.
Two months later, the patient returned to our clinic for a follow-up evaluation of his condition. The facial lesions, rash, and blisters, had almost disappeared but the patient still noted a little pain in the right jaw area, and residual pigmented scars were present (Figure 3B). The dermatologist informed the patient that drugs might be necessary for an extended period of time.
III. DISCUSSION
Herpes zoster occurs when the varicella zoster virus that has remained latent is reactivated6). Herpes Zoster is a less common disease and the factors causing reactivation are still not well known, but it occurs more often in older and/or immunocompromised individuals7).
Clinicians should understand that when herpes zoster involves the mandibular branch, it can mimic a toothache. Because it can appear in the presence or absence of skin lesions, its diagnosis might be difficult for clinicians.
Patients with a herpes zoster infection usually progress through three stages: a prodromal stage, active stage (also called acute stage), and chronic stage8,9). The pain of the prodromal stage, 3-5 days before vesicular eruption2,10), can simulate odontogenic pain. Therefore if there is no convincing evidence of disease of the pulp, unnecessary treatment must be avoided.
In this case report, when the patient visited our clinic presenting odontogenic pain on the lower right mandible, it may have been the prodromal stage with no skin lesions. He complained of pain and a swelling sensation on the lower right mandible. It is believed that these sensory changes are the result of degeneration of nerve fibrils from viral infection activity. This usually precedes the rash of the active stage by a few hours to several days5,8,9).
Ragozziuo et al.10,11) reported that the incidence of trigeminal herpes zoster virus is relatively low, especially in the second and third branch; it only accounts for about 1.7% of all reported cases. In this report, the herpes zoster was involved with the 3rd branch, the mandibular nerve, of the trigeminal nerve. Symptoms mimic odontogenic pain, especially pulpitis in the lower right molars.
For the treatment of herpes zoster, (i) patients with herpes zoster infection should be isolated due to the contagious nature of the infection, (ii) pain should be reduced by analgesics, such as acetaminophen, codeine, and nonsteroidal anti-inflammatory agents, and (iii) antiviral therapy must be swift and precise. Acyclovir has been the drug of choice for a number of years and other antiviral agents, such as famciclovir and valacyclovir, can also be used, (iv) the treatment of post-herpetic neuralgia includes the topical use of capsaicin cream, transcutaneous nerve stimulation, topical anesthetics, injected local anesthetics, and low dose amitriptyline12). Strommen et al.9) offered an in-depth review of the use of antidepressants and neurolyptics in the management of post-herpetic neuralgia.
This case showed that the signs and symptoms of a herpes zoster infection in the mandibular branch can be misdiagnosed. During the prodromal stage, the presenting symptoms may include odontalgia, which may prove to be a diagnostic challenge for the dentist, since many diseases can cause orofacial pain that is similar to pulpitis. Therefore the diagnosis must be established before any invasive treatment, such as endodontic treatment or extraction.


 XML Download
XML Download