

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. INTRODUCTION
During the periapical surgery, root-end cavity preparation and filling procedure following osteotomy and apical root resection should be performed for preventing recurrence of bacterial invasion and infection1). Various materials such as amalgam, zinc oxide eugenol (ZOE), IRM, and super EBA have been used for root-end filling in such situations2). Recently, mineral trioxide aggregate (MTA) became the most popular root-end filling material for its superior sealing ability3,4). MTA was also known to have an excellent biocompatibility. This material can induce the regeneration of periodontium - alveolar bone, periodontal ligament and cementum5-7). Furthermore, it is a material on which the cells can keep their healthy states, grow well and obtain firm attachment8-11). For these reasons, MTA is the material of choice when the root-end filling material is indicated.
Many biologic molecules get involved in wound healing process by several mechanisms. Growth factors and cytokines are mediator molecules that have important roles in tissue development and repair.12,13) Among the mediator molecules, transforming growth factor-beta1 (TGF-β1), fibroblast growth factor-2 (FGF-2), and cytokine interleukin-6 (IL-6) are one of the critical factors. TGF-β1 is known to be related to the mitogenesis of cells and the remodeling of extracellular matrix12,14) while FGF-2 has a potent angiogenic effect15). IL-6 is one of the well-known and plentiful inflammatory cytokines16).
In this regard, Koh et al.17) studied the cytokine production from osteoblastic cells in contact with MTA, and they found that MTA has an up-regulating effect on the expression of IL-1α, IL-1β, and IL-6 from osteoblasts.
Among the cells that constitute the periapical tissue, periodontal ligament (PDL) cells are one of the most abundant and produce many kinds of growth factors and cytokines18). Especially, PDL fibroblasts mainly exist in the periodontal ligaments that encapsulate the cementum of the root, affect the maintenance and regeneration of the periodontal tissue by regulating the turnover of collagen and alveolar bone remodeling, and contact directly with the sealing material when root-end filling procedure is performed19,20). In reference to this, it was reported that PDL fibroblasts can attach and grow well on MTA12).
However, studies regarding the relationship of MTA and growth factors or cytokines from PDL fibroblasts are insufficient. Therefore, the purpose of this study was to monitor the expression of transforming growth factor-beta1 (TGF-β1), fibroblast growth factor-2 (FGF-2), and interleukin-6 (IL-6) from PDL fibroblasts in the presence of MTA.
II. MATERIALS AND METHODS
Preparation of MTA and IRM
100 mg of MTA in white formulae (ProRoot MTA, Dentsply, Tulsa, OK, USA) was mixed with 0.3 mL of distilled water from the enclosed microdose ampoule. For comparison, intermediate restorative material (IRM) (Dentsply, Caulk) was prepared by mixing the same amounts of IRM powder as MTA with liquid according to the manufacturer's instructions. MTA and IRM samples were left to set for 7 days in the sterile well at 37 ℃ under 100 % humidity before cell culture.
Preparation of Cells
The human PDL fibroblasts were obtained from PDL of periodontaly healthy teeth. PDL tissue was cut out with a scalpel from the middle third part of the root surfaces of premolars extracted for orthodontic reasons. The tissue slices were incubated in Dulbecco's modified eagle's medium (DMEM: Life Technologies/GIBCO BRL. Gaithersberg, MD, USA) containing high glucose (4500 mg/L), 10000 U/L penicillin, 10000 µg/L streptomycin, 50µg/L Fungizone (Gemini Bio-Products Inc., Woodland, CA, USA), and 20% heat inactivated fetal bovine serum (FBS) at 37℃ under 5% CO2 and 100% humidity for 2 to 4 weeks. Through trypsinization, cells were removed and transferred into minimum essential medium alpha modification (α-MEM) containing 10% FBS and antibiotics, and continuously cultured. After 5 to 8 cell passages when sufficient cell proliferation was attained, these cells were trypsinized and seeded into the wells on which MTA or IRM had been set. The numbers of cells were 1 × 105 cells per unit well. Then the cells were incubated further for 6, 12, 24, and 48 hours in contact with MTA or IRM (n = 5 per group). The cells seeded and incubated on the wells without material were used as control group.
Enzyme-linked Immunosorbent Assay
Supernatant was collected from samples of each elapsed time in MTA, IRM, and control group and freezed for cold storage for subsequent analysis. After centrifuge (6000 rpm for 5 minutes), we measured the levels of TGF-β1, FGF-2, and IL-6 by enzyme-linked immunosorbent assay (ELISA). Quantikine ELISA kits (R&D systems, Minneapolis, MN, USA) were used for quantitative analysis and the reagents were added according to the manufacturer's instructions. The levels of color development of samples were measured at 450 nm by spectrophotometer (PowerwaveX340, Bio-Tek Instruments Inc., Winooski, VT, USA) and the concentrations of the growth factors and cytokine were determined from the corresponding values of optical density using standard curve. The data were analyzed using one-way ANOVA followed by Scheffe's post hoc test.
III. RESULTS
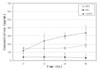
The levels of TGF-β1, FGF-2, and IL-6 production from PDL fibroblasts in all groups are demonstrated in Table 1. Figure 1 shows that the levels of TGF-β1 in all groups are relatively low. At 6 hours, the mean level of TGF-β1 in MTA group was 148.12 pg/mL, which was a little higher than 120.24 pg/mL in control group. Then the level of TGF-β1 in control group was increased and kept higher values than those in MTA group after 12 hours, and the differences were significant at 24 and 48 hours (p < 0.05). The production of TGF-β1 showed a tendency to increase with time in control group, and kept relatively constant level in MTA group. The expressions of TGF-β1 in IRM group were significantly suppressed and hardly detectable at all time points checked (p < 0.05).
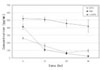
The data of FGF-2 are expressed in Figure 2. The levels of FGF-2 production at 6 hours were 260.92 pg/mL in MTA group, 413.27 pg/mL in IRM group and 522.51 pg/mL in control group, with the highest value in control group and the lowest in MTA group. At 12 hours, the levels of FGF-2 in MTA and IRM group were decreased to 160.47 pg/mL and 107.27 pg/mL respectively, and kept declining with time thereafter. The levels in MTA group kept higher values than those in IRM group after 12 hours, but the differences were insignificant at 24 and 48 hours. The levels of FGF-2 in both experimental groups were significantly lower than that in control group at all time points observed (p < 0.05).
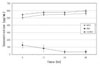
The graph in Figure 3 describes the levels of IL-6. The concentrations of IL-6 in MTA group were comparable to those in control group at all time points checked. No obvious variation with time was observed. The expressions of IL-6 in IRM group showed significantly decreased levels compared to those in two other groups throughout the experiment (p < 0.05).
IV. DISCUSSION
The dentoalveolar healing mechanism after periradicular surgery is not fully revealed. After the resection of the apical portion of the root and the placement of root-end filling material, undifferentiated mesenchymal cells, fibroblasts, and fibroblast-like cells egress from the bone and periodontal ligament and these cells surround the root end to begin the healing process21,22). When it was used as a root-end filling material, fibrous connective tissue and thin layer of hard tissue formed in direct contact to MTA7,23). It is due to its low cytotoxicity against human PDL fibroblast, and for this reason, it is recommended to use of MTA in the root-end environment24). In this regard, we hypothesized that new root-end filling material MTA would influence the healing of tissues by modulating the production of growth factors and cytokines from PDL fibroblasts. Growth factors are known to be the essential molecules that act in the host defense and tissue regeneration25). Extensive wound healing studies in relation to growth factors demonstrated that TGF-β1 and FGF can promote tissue repair26). These mediators regulate hard and soft tissue healing mechanism by inducing recruitment, proliferation and differentiation of specific cells. It was reported that TGF-β1 stimulates the proliferation and differentiation of osteoblasts and induces bone formation27,28), however, its effects on bone healing appear inconsistent. Regarding the soft tissue healing, Okuda et al.29) demonstrated that this growth factor stimulated the biosynthesis of extracellular matrix components such as type I collagen, proteoglycan, glycosaminoglycan, and fibronectin. TGF-β1 also appears to inhibit the formation of extracellular matrix degrading protease and as a result it enhances the formation of granulation tissue. Takayama et al.30) have reported that FGF-2 influenced extracellular matrix formation by accelerating human endothelial cell migration and proliferation. It is also reported that FGF-2 potently stimulates angiogenesis which is critical for granulation tissue formation15). Our result suggests that MTA plays an important role in the process of periapical tissue healing by suppression of granulation tissue formation ability of these growth factors produced from PDL fibroblast. The similar molecules related to the tissue repair are called cytokines. Some authors do not discriminate cytokines from growth factors and consider them as the same category14). Main functions of cytokines are the recruitment and activation of immune and inflammatory cells. They activate the defensive mechanisms of host and prepare the basis for tissue regeneration. The cytokine IL-6 is an essential factor in protective response to injury and bone remodeling in wound healing31). From our result that there was no difference in expression of cytokine IL-6 in the presence of MTA compared to control indicates that bone remodeling mediated by IL-6 is undisturbed during periapical tissue healing process when PDL fibroblasts are grown in contact with MTA. This is in agreement with recent study showing that IL-6 was not produced by mouse fibroblast and macrophage cells cultured on MTA32). In the present experiment, positive control IRM was also shown to suppress growth factor expression. Therefore, it seems that there is no difference between MTA and IRM in their ability of modulating growth factor production from the PDL fibroblasts. However, IRM inhibited not only growth factors but also cytokine expressions from the cells. Koh et al.33) reported same result that cytokines such as IL-1α, IL-1β, and IL-6 were not produced from the osteoblast in the presence of IRM. It is thought that the toxicity of IRM totally suppressed the biologic function of cells and this phenomenon is mainly due to the well-known cytotoxic effect of this material. This result supports the use of MTA for the root-end filling material. The ideal goal of priradicular surgery is the complete healing of periapical tissue. We presume that root-end filling material MTA inhibits the stimulatory function of growth factors TGF-β1, FGF-2 on granulation tissue formation and in turn, it promotes the healing process modulated by other bone-remodeling cells. However, the effect of these growth factors in the presence of MTA on each type of cell population in the periapical tissue that is involved in tissue repair has not been fully clarified yet. It is hoped that the result of this study will provide valuable information for the better understanding of possible role of MTA as a root-end filling material in periapical tissue regeneration.
V. CONCLUSION
MTA significantly suppressed the productions of TGF-β1 from PDL fibroblasts compared to control group at 24 and 48 hours (p < 0.05).
MTA significantly down-regulated the expressions of FGF-2 at all time points checked (p < 0.05).
MTA showed little effect on the expressions of IL-6 throughout the experiment (p > 0.05).

 XML Download
XML Download