

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. INTRODUCTION
The loss of hard tissue in the cervical region of the tooth is a common clinical occurrence1). These noncarious cervical lesions (NCCLs) can occur on facial, lingual and/or interproximal surfaces. Traditionally, this has been assumed to be due to the effects of abrasion and/or erosion1-3). More recently, an additional mechanism for cervical tooth loss with occlusal loading has been proposed2,4). Grippo3) has coined the term "abfraction" to distinguish it from lesions caused by erosion and abrasion.
Clinically, there is some clinical evidence for the association of abfraction lesions with heavy occlusal loads. There is a marked association of these lesions with bruxism and malocclusion5). Some epidemiologic studies also reported a strong association between cervical lesions and occlusal tooth wear or occlusal erosion with 96% of teeth with a cervical lesion also having evidence of occlusal pathology6). These lesions have been shown in teeth subjected to lateral load, but adjacent teeth that were not subjected to these forces remained unaffected7).
Abfraction lesions are sharp, angular, wedge-shaped defects that sometimes have a subgingival location and are often associated with occlusal wear facets7-9). These lesions are commonly observed on the buccal and labial aspects of the teeth. These lesions were rarely found on the lingual surface with one study reporting that only 2% of cervical lesions were found lingually6).
There is a gradually increasing body of evidence to suggest that the effects of occlusal loading contribute to the development of abfraction lesions. This evidence comes from various types of stress and strain analysis including photoelastic stress analysis, strain gauge studies and finite element analysis (FEA).
Selna and co-workers10) revealed through 2D FEA that eccentric load application demonstrated internal stress distribution in the crown and roots, which may be interpreted as possible failure planes both in the dental structures and restorations. Yettram and co-workers11) showed that the occlusal load on a mandibular second premolar flowed around enamel cap and through the thin enamel cervical area before being transmitted to the root in their 2D FEA. Goel et al.12) used the 3D FE model of the maxillary first premolar. The magnitude of normal stresses increased at the cervical enamel and the normal stress and shear stress were markedly affected by the contour of the dentinoenamel junction (DEJ) and the thickness of the occlusal third on the buccal and lingual surfaces.
Palamara et al.13) used the model 3D FEA of a mandibular second premolar to investigate the effects of occlusal load on enamel surface. Point loads of 100N were applied axially at the 45° from the vertical at the cusp. Strains predicted from the FEA model were in excellent agreement with the strain gauge measurements. Strains were concentrated near cementoenamel junction (CEJ) regardless of load direction. Rees14) developed 2D FEA of a maxillary incisor, canine and first premolar and the cervical stress profiles were examined along a horizontal plane 1.1 mm above the CEJ. The result of 500 N loaded 45° labioapically to the incisal tip was that the stress profile in the cervical region of central incisor was greater than the canine or premolar. Tanaka et al.15) carried out stress analysis on the upper central incisor and the lower first molar using the plastic-elastic deformation theory with 2D FEA. The result was that oblique loading causes plastic deformation near the CEJ. Geramy and Sharafoddin16) developed 3D FEA of a maxillary central incisor including periodontal ligaments and alveolar bone, which was loaded 1.5 N static non-axial and axial loads on the palatal side. The maximum displacement and stresses were shown at the cervical area on the non-axial load, but the axial load did not show the same.
In the previous study of 2D FEA, the results are unreliable for assessment of stress patterns due to its inability to duplicate tooth geometry. Further refining the 3D FE model shape was important when analyzing the stress distribution within a tooth. The objective of this study was to investigate the effects of various occlusal loads on the stress distribution of the buccal cervical region of a normal maxillary second premolar, using a 3D FEA.
II. MATERIALS AND METHODS
Finite element model
For developing a 3D FE model to analyze, an intact normal extracted human maxillary second premolar was selected in this study. The premolar was scanned serially with Micro-CT (SkyScan 1072; SkyScan, Aartselaar, Belgium) to exposure the tooth sections perpendicular to the long axis of the tooth (58 µm in thickness) and parallel to the occlusal plane. 3D-DOCTOR (Able Software Co., Lexington, MA, USA) image processing software was employed to detect the boundaries of enamel, dentin and pulp from the sectioned two dimensional images and to make a three-dimensional surface model. Rhino 3D (Robert McNeel & Assoc., Seattle, WA, USA) was used to reduce useless nodes from the surface model and ANSYS (Swanson Analysis Systems, Inc., Houston, USA) was used to mesh.
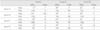
The 3D FE model was consisted of hexahedral elements. The final model consisted of 15,608 elements with 17,052 nodes. All the vital tissues were presumed linearly elastic, homogeneous and isotropic. The corresponding elastic properties such as Young's modulus and Poisson's ratio were determined according to literature survey (Table 1).
The periodontal ligament was assumed to be 0.3 mm wide, and the dimensions of surrounding compact and cancellous bone were derived from standard texts18,19). The alveolar bone was also generated by growing the outer surface of the tooth model from 2 mm below the CEJ18,19). The pulp region was modeled as being hollow20). In these models, the outer surface of the alveolar bone model was fixed in order to prevent rigid body motion for FEA.
The model was fixed on mesiodistal direction. In all loading cases, the base nodes of simulated alveolar bone were assumed fixed to prevent rigid body motion.
Loading conditions
Static 500 N forces were applied for the following three loading conditions (Figure 1). The eccentric occlusion was simulated with two loading conditions. Load-I represented the perpendicular load at the point of upper third of palatal incline of buccal cusp. Load-II represented the perpendicular load at the point of upper third of buccal incline of palatal cusp. And the centric occlusion was simulated with Load-III. Load-III represent a unit load distributed at the three points corresponding to centric occlusion(A: perpendicular load on the lower third of palatal slope of buccal cusp, B: perpendicular load on the buccal slope of palatal cusp, C: perpendicular load on the center of mesial marginal ridge).
Stress analysis
Analysis of the principal stresses has been done by ANSYS.
The values of maximum and minimum principal stresses of thirteen nordal points in the buccal cervical region were sampled along four horizontal surface enamel planes (Level A, B, C, and D) and two horizontal DEJ planes (Level A, B). The Level of CEJ was designed as Level C and which was used as reference plane. Level A and B were the plane of 1.0 mm and 0.5 mm above the CEJ level, respectively. And the Level D was 0.5 mm below the CEJ.
III. RESULTS
Principal stress analysis
Cervical stress contours on the tooth surface in response to a static point 500 N load are shown in figure 2.
The principal stresses of Level A (Figure 3)
The principal stresses were different in magnitude and character according to the load conditions.
In Load-I case, the peak tensile stress of 17 MPa at the mid-buccal and the peak compressive stress over the 144 MPa at the mesial side were observed. But in Load-II case, the peak tensile stress of 49 MPa was concentrated at the mesiobuccal line angle area. And in Load-III case, tensile stress of 21 MPa at the distal side and the peak compressive stress of 121 MPa at the mesial side were observed.
The principal stresses of Level B (Figure 3)
Peak compressive stress of 152 MPa was concentrated at the mesiobuccal line angle area in Load-I case. And peak tensile stress of 59 MPa at the mesiobuccal line angle area in Load-II case. In Load-III case, peak compressive stress of 118 MPa at the mesiobuccal line angle and peak tensile stress of 32 MPa at the distobuccal line angle were detected.
The principal stresses of Level C (Figure 3)
In Load-I case, the peak tensile stress of 20 MPa at the distal side and the peak compressive stress over the 226 MPa at the mesiobuccal line angle area were observed. But in Load-II case, the peak tensile stress over the 101 MPa was concentrated at the mesiobuccal line angle area. And in Load-III case, the tensile stress was particularly observed between the mid-buccal and the distal CEJ. The peak tensile stress of 41 MPa at the distal CEJ and the peak compressive stress of 144 MPa at the mesial CEJ were observed.
The principal stresses of Level D (Figure 3)
In Load-I case, the peak tensile stress of 51 MPa at the distal root surface dentin and the peak compressive stress over the 97 MPa at the mesiobuccal line angle area were observed. But in Load-II case, the peak tensile stress of 49 MPa was observed at the mesiobuccal line angle area. And in Load-III case, the peak tensile stress of 51 MPa at the distal root surface dentin and the peak compressive stress of 55 MPa at the mesial side were observed.
IV. DISCUSSION
The etiology of NCCLs has not been precisely defined. Most authorities agree that the cause is multifactorial and thus difficult to recognize22). The most frequent causes are erosion, abrasion and occlusal loading. Occlusal stresses are the primary cause in traumatic occlusion and bruxism can produce cervical lesions23). When eccentric occlusal forces are applied to a tooth, both compressive and tensile stresses are placed on the structure. The stress produced causes the tooth to flex. This has been proposed as a tooth flexure theory by Levitch et al.24). The fulcrum of this bending movement and the place where eccentric occlusal forces are concentrated is the cervix of the tooth. The location of the fulcrum determines the exact site of the lesion24). A longitudinal case study25) of a person showed a direct correlation between occlusal wear and the growth of NCCLs. Heymann et al.26) also found a relationship between the loss of cervical restorations and the presence of a traumatic occlusion, which is expected to cause more cuspal flexure.
In order to determine the load conditions such as magnitudes, directions, occlusal contacts (i.e., point or surface, centric or eccentric), preliminary investigation was performed using the data gathered by literature review27,28). Based upon these data, 170 N was assumed as the chewing force for premolars and 500 N was assumed as the heavy parafunctional load of bruxism and traumatic occlusion. In this study, a tooth model loaded by a point load of static 500 N was considered more representative of high-risk loading situation, in contrast to other FEA studies11-16). Load-I for buccal eccentric occlusion and Load-II for palatal eccentric occlusion were selected. Load-III was selected for mimicking the effect of a unit load in centric occlusion.
The peak stress was seen asymmetrically at the CEJ of mesiobuccal line angle area. The position of maximum stress concentration found in this study was different from previous studies29-32). This pattern of stress distribution may be related to the anatomical asymmetry. Palamara et al.13) reported that strains resulting from oblique loads on buccal cusp inclines were asymmetric.
The position of the peak stress found in this study was at the CEJ. Many studies11,13,15,16,29-31) reported that the peak stress was concentrated at the CEJ in their FEA models. Kuroe et al.32) also confirmed by the photoelastic method that a vertical force loaded on the tooth causes stress concentration at the cervical line.
Contrary to our results, Rees et al.4,14,33-35) proposed that the sampling horizontal planes were chosen at 1.1 mm above the CEJ among the buccal cervical region because an initial pilot study showed this to be the position of maximum stress concentration. Despite their findings, the results of their study must be interpreted with a certain amount of caution. First, their analysis was a 2D FEA so it was not possible to model any small twisting movements of the tooth in the Z-axis direction. Second, their study modeled a buccolingual slice through the center of the tooth and therefore represents the worst possible case, since they assumed that teeth flex more in the middle. They thought that a more mesially or distally placed slice would give less cuspal flexure and, presumably, lower cervical stresses. However, in our study, mesiobuccal line angle area was greater than mid-buccal area under 3D FEA model.
Several studies have shown that enamel and dentin are less resistant to tensile stress than compressive stress36-39). In compressive stress, enamel can withstand forces up to 35 times greater than when subjected to tensile stress; meanwhile, dentin can resist compressive forces at least seven times greater than the amount of tensile stress that will cause it to fail37, 38). The tensile strengths of enamel and dentin are much lower than are their respective compressive strengths38,39).
According to the experiment, tensile stress affected the result to the meaningful level while the effect of compressive stress was not. For in terms of Level A, B, C, and D, the peak compressive stress was under the failure stress of the enamel but the peak tensile stress observed 4 times as much as the failure stress of the enamel.
As the results of the evaluation of the principal stresses, it has been shown that the tensile stress on the buccal CEJ regions was dominant in the lesion initiation. This results are similar with Tanaka et al.15) which they reported that when the force was oblique, plastic deformation of the lower first molar appeared at the enamel surface along the cervical region because of the tensile stress. Spears et al.40) showed that a vertical force loaded at one tip of the lingual cusp of the mandibular second premolar produces tensile stress at the lingual enamel on the cervical region. Borcic et al.31) reported that in their 3D FEA model, large tensile stress appeared on the enamel surface near the cervical line at the side opposite the loading point.
This study reports a strong association between loading forces of Load-II and the possibility of failure of enamel and dentin of the buccal cervical area by tensile stress -the same as other studies15,29,31). Since the tensile stress of Load-II was 101 MPa, the highest level on the CEJ, Load-II is thought to be the most damaging factor. Lee and Eakle7) also proposed that the primary etiologic factor in wedge-shaped cervical lesions is tensile stress from mastication and malocclusion, and that local factors may play a secondary role in the dissolution of tooth structure.
We adopted Load-III mimicking centric occlusion as control group in order to compare it with the eccentric occlusion. Unexpectedly, Load-III generated tensile stress enough to destroy enamel on the distal CEJ. In these results, we came to conclusion that tensile stress generated from the centric occlusion may be related to the formation of NCCLs in a significant level. Not only eccentric occlusion but also centric occlusion seems to be related with the formation mechanism of NCCLs clinically observed in the buccal CEJ, the Level C, and they seems to generate stress concentration working together.
Grippo41) said that the high incidence of cervical abfraction lesions in Koreans is noteworthy and warrants investigation in his suggestions for future studies. But it is hard to find the epidemiologic study reported a strong association with a NCCLs and occlusal tooth wear except for one Korean study42). It is necessary to have further clinical study for NCCLs of Koreans together with epidemiologic study and this study of 3D FEA using the maxillary second premolar of a Korean might be the preliminary research.
V. CONCLUSIONS
1. The peak stress was seen at the cervical enamel surface of the mesiobuccal line angle area, asymmetrically.
2. The values of compressive stresses were within the range of the failure stress of enamel. But the values of tensile stresses exceeded the range of the failure stress of enamel.
3. The tensile stresses from the perpendicular load at buccal incline of palatal cusp may be shown to be the primary etiological factors of the NCCLs.





 XML Download
XML Download