

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. INTRODUCTION
The complete filling of a root canal system is one of the most important aspects of a successful endodontic treatment. Ingle et al.1) reported that approximately 60% of endodontic failures are related to incomplete filling of the root canal. The integrity of the apical seal depends on mechanical preparation, irrigation, filling technique, type of root canal sealer, and the intracanal medicament.
Since its introduction by Hermann in 1920 calcium hydroxide (Ca(OH)2) has been widely used in endodontics. It is a strong alkaline substance, which has a pH of approximately 12.5. In an aqueous solution, Ca(OH)2 dissociates into calcium and hydroxyl ions2). Various biological properties have been attributed to this substance, such as antimicrobial activity3), tissue-dissolving ability4,5), inhibition of tooth resorption6), and induction of repair by hard tissue formation7). Because of such effects, Ca(OH)2 has been recommended for use in several clinical situations8,9). Currently, this chemical substance is acknowledged as one of the most effective antimicrobial dressings during endodontic therapy.
Ca(OH)2 needs to be completely removed from the canal in order to obtain a hermetic seal of the permanent root canal filling10,11). It has been suggested that the Ca(OH)2 remnants be removed by increasing the instrumentation of the medicated canal by one or two file sizes12). However, the effectiveness of these procedures has not been fully documented. Therefore, this study investigated the difference in apical leakage between teeth where two different Ca(OH)2 removal techniques were used.
II. MATERIALS AND METHODS
Seventy extracted human permanent teeth with single canals and mature apices were used in this study. The teeth were stored in a 0.9% isotonic saline at room temperature. The specimens were soaked in 5.25% NaOCl for 30 min, and the remaining periodontal tissue and calculus were removed. In order to facilitate instrumentation, the crown portion of each tooth was removed using a diamond-cutting bur.
The working length was determined by placing a #10 K file (K-flexofile, Dentsply Maillefer; Ballaigues, Switzerland) until it was just observed penetrating the foramen, after which 1 mm was subtracted and the length was then recorded. The canals were prepared using Profile rotary files (Profile .06, Dentsply Maillefer; Ballaigues, Switzerland) to a #30 at the working length. Irrigation with 5.25% NaOCl solution was performed using a MAX-I-Probe (MAX-I-Probe, Dentsply Maillefer; Ballaigues, Switzerland) during the instrumentation.
After completing the instrumentation, the canals were dried with paper points. Fifty-eight teeth were filled with calcium hydroxide paste (Metapaste, Metadent Co., Chongju, Korea) according to the manufacturer's instructions. Twelve teeth were left as positive and negative controls. The coronal 3 mm of all the canals were sealed with Cavit. The teeth were wrapped in a water-saturated 2 × 2-inch gauze, and placed in an incubator at 37℃.
After 1 week, the Cavit was removed from the canals. In group A (29 teeth) : The canals were irrigated with 5 ml of a 5.25% NaOCl solution and a #10 patency file was used to remove the residual Ca(OH)2 paste. In group B (29 teeth): The canals were prepared with a Profile rotary file-one size larger (#35) than previous one used at the working length and were irrigated with 5 ml NaOCl irrigation (Table 1). In the positive control group (6 teeth) : the canals were not obturated after the canal preparation. In the negative control group (6 teeth): The prepared canals were obturated with gutta-percha and an AH-26 sealer, and two coats of nail varnish were applied to the whole root surface. All the specimens except the positive control group were obturated by a continuous wave of condensation techniques with gutta-percha points and AH-26 sealer after paper point drying.
For all specimens, the coronal gutta-percha was removed, leaving only the apical 4 mm of the root filling material. Copper wires, which were used as the experimental electrodes, were inserted into the canals in contact with the remaining gutta-percha. Approximately 0.5 cm of the insulation coat was stripped off at both ends of the wire. A small piece of the red sticky wax was adapted around the wire at the occlusal opening to stabilize the wire.
All the specimens except the negative control specimens were coated with double layers of nail varnish from the CEJ to the area 4 mm away from the apex. All the specimens were set in bottles. The copper wire was extended to the outside of the bottle cap. Stainless-steel wires were placed at the center of the caps as standard electrodes. A 0.9% NaCl solution was placed in the bottles as an electrolyte until the apical half of the roots were covered (Fig. 1).
The electrical resistance between the standard and experimental electrodes was measured using a multitester (Dagatron 2021, Dagatronics Corp., Seoul, Korea). The resistance was measured once a day for 24 days. The raw data was recorded and analyzed for statistical significance using repeated measures of ANOVA.
III. RESULTS
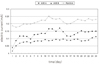
Increasing apical leakage with time was observed in all the groups except for the negative control group. The mean apical leakage of the data is illustrated in Fig. 2. The leakage increased markedly within the first three days. There was a slight increase in all the groups throughout the test period. No apical leakage was observed in the negative control group. The positive controls showed leakage immediately after the experiment. Group A exhibited a tendency to show more apical leakage than group B. However, there was no statistically significant difference between groups A and B (p > 0.05).
IV. DISCUSSION
Many studies have examined the effect of a calcium hydroxide dressing on apical leakage in root canal therapy. As a general rule, calcium hydroxide should be completely removed from the canal in order to hermetically seal the permanent root canal filling. Ricucci and Langerland10) reported a case where the incomplete calcium hydroxide removal from the root canal caused endodontic failure. In addtion, Lambrianidis et al.11) investigated the removal efficiency of a calcium hydroxide dressing from the root canal and suggested the potential problem of calcium hydroxide retention. Webber et al.12) suggested that all the calcium hydroxide remnants should be removed by increasing the instrumentation of the medicated canal to the files one or two sizes larger than the one used at the working length.
In this study, it was found that there were no significant differences in the apical leakage levels with the two removal methods studied. However, this study was conducted using the teeth with large and straight single canals so the irrigation needle could easily access the apex. In addition, the smooth canal walls prepared by the Profile make removal of calcium hydroxide by irrigation from the root canal wall easier. The effect on teeth with small and curved canals should be evaluated. Moreover, it would be better if a SEM examination or image-processing analysis could be used to compare the calcium hydroxide removal techniques.
Porkaew et al.13) reported that the residual Ca(OH)2 along the root canal walls enhanced the sealing quality of the root canal filling. Holland et al.14) reported a similar result. Porkaew et al.13) suggested two possible explanations. One explanation is that the residual Ca(OH)2 may have been incorporated into the sealer during obturation and might have caused a decrease in the permeability of the sealer itself. Another possibility may be that Ca(OH)2 was transported or mechanically forced into the dentinal tubules, which occluded the dentinal tubules. However, also reported that Ca(OH)2 can react to form calcium carbonate that is absorbable, and this will most likely create voids at the root/filling interface in the long run. Therefore, the improved initial apical seal found in the short-term in vitro study may be temporary. In the above two studies, methylene blue (MB) dye was used as leakage tracer. In a study by Wu et al.15), 1% MB dye solution became greatly decolored after being in contact with calcium hydroxide for 24h. Therefore, the penetration of the MB solution observed along the root canal filling following the root canal dressing could be underestimated. Kontakiotis et al.16) reported using the fluid transport model that no significant difference was found between the two groups where one group received calcium hydroxide dressing and the other did not.
As this study was an in vitro study and the test period was short, so there was insufficient time to resolve the residual calcium hydroxide, as is the case in clinical situations.
The electrochemical method was used in this experiment. Jacobson and von Fraunhofer17) described this technique for measuring microleakage. Delivanis and Chapman18) found this method to be effective and reliable. They reported that the electrochemical method could provide a quantitative measurement of the apical leakage and the opportunity to study over a continuous time period.
This technique is based on the principle that an electric current will flow between two pieces of metal when both are immersed in an electrolyte and are connected by an external power source. In this study, one piece of metal (stainless steel wire as the standard electrode) was immersed in a 0.9% sodium chloride solution (electrolyte), and the other piece of metal (copper wire as the experimental electrode) was placed in the coronal portion of an endodontically treated tooth. When leakage occurs, an electrolytic pathway is established between the copper and the stainless steel electrodes. The magnitude of the current that flows can be used to measure the degree of microleakage. This is because the current magnitude is controlled by the degree of electrolyte diffusion to the electrode surface, which is directly proportional to the surface area of the electrode. In this study, the magnitude of the current was measured as the electrical resistance between the standard and experimental electrodes. The advantage of this technique over previously used methods for testing leakage is that it can be monitored continuously throughout the test period and both the number of leaking teeth and the degree of leakage can be determined. The fluid filtration method present similar advantages over the dye penetration method: the samples are not destroyed, permitting measurement over time, no tracer needed. However it showed the need for standardization to compare the results from various syudies19). Pommel and Jacquot20) compared three methods (Dye penetration, fluid filtration, electrochemical), and reported that several studies using various methods were necessary before comparing the apical leakage.
The Repeated Measures of ANOVA used in this study is the statistical method for testing difference between groups for repeated measures data. Schuurs and Wu21) described the power and the statistical related factors that determine the adequate size of samples. They reported that the use of small sample sizes might imply that a rather large difference between two mean leakage scores is not found to be significant, thereby leading to incorrect conclusion. It may be need to another study that use more samples than this time.
The use of calcium hydroxide in root canal therapy has already been established. It has many advantages, but only possible problem may be if residual Ca(OH)2 compromises the seal. Further studies on the methods of calcium hydroxide removal in addition to the effects of residual calcium hydroxide utilizing the various evaluation methods resembling various clinical situations will be needed.
V. CONCLUSION
The technique of a one-size larger filing and irrigation with a 5.25% NaOCl solution is slightly superior to the one irrigating with a 5.25% NaOCl solution and using a #10 K-file as a patency file to remove the residual calcium hydroxide paste. However, there was no statistically significant difference between the two calcium hydroxide paste removal techniques. In addition, there was a tendency for the amount of leakage to increase with time. In a straight canal, there is no point further enlarging canals and further weakening the tooth in a vain attempt to remove the Ca(OH)2.


 XML Download
XML Download