

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. INTRODUCTION
After root canal system is cleaned and shaped, it needs to be obturated hermetically to eliminate all avenues of leakage from the oral cavity or the periradicular tissues into the system and to seal within the system any irritants that cannot be fully removed1).
Various techniques and instruments have been developed in an attempt to improve the quality of root canal treatment in curved canals2-5). Advances in instrument design and material have resulted in the development of various tapers of nickel-titanium endodontic instruments and gutta-percha cones.
ISO standardization describes a taper of 0.02 for both endodontic instruments and gutta-percha cones6). Hence, 0.02 taper gutta-percha cones have been recommended to use in the canals prepared with 0.02 taper endodontic instruments. Since various tapers of endodontic instrument have been introduced recently, various tapers of gutta-percha cone may be used in the canals. Canals prepared with recently introduced nickel-titanium instruments can be obturated using a variety of warm vertical or lateral compaction techniques. To take advantage of the more flared canal preparation produced by more tapered instruments than standardized files7), a correspondingly tapered non-standardized gutta-percha cone may be used as a master cone8). For the canals prepared with 0.06 tapered instruments, use of non-standardized size medium gutta-percha cones that have a 0.054 taper9) would be expected to meet such a criteria10) efficiently.
The purpose of this study was to evaluate the obturation efficiency of a non-standardized gutta-percha cone when cold lateral compaction technique was employed in curved root canals prepared with 0.06-tapered nickel-titanium instruments.
II. MATERIALS AND METHODS
Sixty simulated root canals in clear resin blocks (REF A 0117, Dentsply Maillefer, Ballaigues, Switzerland) were used, which have 34 to 35 degree curves and a mean canal length of 18 mm.
Before using rotary nickel-titanium files for the preparation of the root canal, all canals were explored with stainless steel size 10 K-files and their working lengths were established 0.5 mm short of the apical foramen. Canals were instrumented with two rotary nickel-titanium file systems (ProTaper™ and ProFile®, Dentsply-Maillefer, Ballaigues, Switzerland). Coronal two-thirds of the canal was prepared with ProTaper™ according to the manufacture's recommended sequences. Shaping file No. 1 (S1) was used with moving apically to just short of the working length (16 mm). SX file was then used to resistance (13 to 14 mm). Files S1 and S2 were taken to working length. When the coronal two-thirds of the canal had been prepared, the apical one-third was instrumented with ProFile®. After the confirmation of the canal patency, apical canal was prepared with size 15 of 0.04 taper, followed by sizes 20 and 25 of 0.04 taper, size 25 of 0.06 taper, size 30 of 0.04 taper, and finished with size 30 of 0.06 taper. Root canals were irrigated with water after the use of each instrument. RC-Prep™ (Stone Pharmaceuticals, Philadelphia, USA) was used as a lubricant. All canals were dried with paper points.
Prepared sixty root canals were randomly divided into four groups of fifteen canals. For canal obturation, two different master cones and two different finger spreaders were used: an ISO standardized size 30 gutta-percha cone and a non-standardized size medium gutta-percha cone (Diadent, Chongju, Korea) after matching the apical size of 30 with a cone gauging device, type B stainless steel and nickel-titanium finger spreaders (Dentsply-Maillefer, Ballaigues, Switzerland). All canals were obturated with cold-lateral compaction technique and AH 26® sealer (Dentsply-DeTrey, Konstanz, Germany) using the following master gutta-percha cone and spreader: a standardized size 30 cone and a stainless steel spreader in St/SS group, a standardized size 30 cone and a nickel-titanium spreader in St/NT group, a non-standardized size medium cone and a stainless steel spreader in Non-St/SS group, and a non-standardized size medium cone and nickel-titanium spreader in Non-St/NT group (Table 1).
After placing the root canal sealer in the canals with a lentulo spiral, the master cones were coated with sealer and seated. In each canal, root canal spreader was inserted to 2 mm from the working length for the first accessory cone and to the possible deepest point for the additional accessory cones with finger pressure. Type A accessory cones (Dentsply-Maillefer, Ballaigues, Switzerland) were added to all canals until a finger spreader no longer penetrated deeper than the coronal one-third of the canal. Excess gutta-percha was removed with a heated endodontic plugger, and the gutta-percha in the canal orifice was vertically condensed. Number of accessory cones was counted that were used to finish the obturation in each group.
All resin blocks were stored in a humidor at 37℃ and 100% humidity for setting of the sealer and were cross-sectioned at 1, 3, and 5 mm levels from the apical foramen with a microtome (Isomet™, Buehler Co., Lake Bluff, IL, USA). Each section was photographed under a stereomicroscope (SZ40, Olympus Optical Co. Ltd., Tokyo, Japan), and stored in a computer using a CCD camera (GP-KR222, Panasonic, Osaka, Japan) and a commercial digitizing image program (miroVIDEO Studio 200 program, Pinnacle system, Brauschweig, Germany).
After tracing the periphery of the root canal and gutta-percha cone area using a digitizer (Intuos™, Wacom Company Ltd., Saitama, Japan), the ratio of gutta-percha area in the cross-sectional area of the canal were calculated using a computer program (Auto®Cad 2000, Autodesk Corp., San Rafael, CA, U.S.A.) at each apical levels.
Data of gutta-percha area ratio were analyzed with two-way ANOVA. Data of number of accessory cones were with one-way ANOVA and Duncan's multiple range test. p value of less than 0.05 was regarded significant.
III. RESULTS
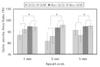
Figure 1 shows cross-sectional views of canal at each level and Figure 2 shows the ratio of gutta-percha area at each level in different groups. At apical 1 mm level, the mean ratio was 86.67 ± 3.24% (mean ± S.D.) in St/SS group, 91.86 ± 2.87% in St/NT group, 94.33 ± 2.43% in Non-St/SS group, and 94.04 ± 2.86% in Non-St/NT group. Non-standardized cone groups showed significantly higher ratio than standardized cone groups (p < 0.01).
At apical 3 mm level, the mean ratio was 81.55 ± 7.18% for St/SS group, 85.66 ± 5.56% for St/NT group, 93.35 ± 7.42% for Non-St/SS group, and 95.54 ± 1.57% for Non-St/NT group. Non-standardized cone groups showed significantly higher ratio than standardized cone groups (p < 0.01).
At apical 5 mm level, the ratio of gutta-percha area was 91.19 ± 4.46% for St/SS group, 86.48 ± 5.04% for St/NT group, 94.47 ± 3.48% for Non-St/SS group, and 94.75 ± 2.39% for Non-St/NT group. Non-standardized cone groups showed significantly higher ratio than standardized cone groups (p < 0.01).
Results for number of accessory gutta-percha cones are summarized in Figure 3. Non-standardized cone groups used significantly less accessory cones than standardized cone ones (p < 0.01).
IV. DISCUSSION
For long term success, root canal system needs to be filled with as much solid core material, which resists absorption, as possible and as little absorbable paste as possible11-13).
With the use of varying tapered instruments to prepare root canal, the resultant taper of the canal will be affected. Filling canals prepared by nickel-titanium instruments with a correspondingly tapered gutta-percha master cone will be advantageous because it will be clinically efficient and seems to result in a radiographically acceptable outcome8).
Even though ISO-standardized 0.02 tapered master gutta-percha cones have been used in lateral compaction technique14), non-standardized gutta-percha cones may be used as a master cone in lateral compaction technique in canals prepared with non-standardized instruments. The results of the present study demonstrated that canals prepared with 0.06 tapered nickel-titanium rotary instruments were more effectively and efficiently obturated with the use of non-standardized size medium master gutta-percha cone than with ISO-standardized 0.02 tapered master gutta-percha cone when lateral compaction technique was used.
Taper of the non-standardized size medium master gutta-percha cone, which was used in the present study, was 0.054. This taper matches or closely matches the taper of the rotary instruments used for preparation10). Because lateral compaction, unlike vertical compaction, does not create a homogeneous mass of gutta-percha, pools of sealer may be trapped in the filling mass as accessory cones are compacted against each other. Filling with a master cone with a larger taper may be advantageous in that a larger and more uniform mass of gutta-percha is introduced that potentially has less sealer entrapped in the filling mass.
The ProFile 0.06 rotary instruments produced a uniformly round prepared canal space in all specimens which Glossen et al.15) demonstrated that engine-driven, nickel-titanium instruments produced rounder and more centered preparations than did hand instruments. It seems from the results of this study that size medium gutta-percha cones conform better to these round, tapered spaces than do ISO-standardized gutta-percha cones, and thus require fewer accessory cones when used as master cones in the lateral compaction technique.
On the observation of the cross-sectioned specimen, the prepared canal space in all specimens of non-standardized cone groups appeared to contain one master gutta-percha cone only at apical 1 mm level, and one master cone and one, two or three accessory gutta-percha cones at apical 3 and 5 mm levels with minimal or little sealer present at the gutta-percha/canal wall interface. These findings may be attributed to the fact that custom-fitted, size medium master cones, having a nearly equivalent taper to that of the ProFile 0.06 instruments used to prepare the space, also had the similar diameter at this level as did the space prepared by these instruments. In contrast, the ISO-standardized master cone with its smaller taper of 0.02 taper had a smaller diameter at this level than the prepared canal space. Thus, in the specimens of standardized cone groups, there was sufficient room for both spreader penetration and seating of accessory cones at these levels. These findings are also consistent with the number difference of accessory cone used in the present study.
Most authors evaluate obturation quality by determining the amount of apical or coronal microleakage that occurs in obturated specimens. This microleakage may occur at the interface of the dentin and sealer, at the interface of the solid core and sealer, through the sealer itself, or by dissolution of the sealer. Leakage does not occur through the solid core16). The goal of obturation should therefore be to maximize the amount of solid core and minimize the amount of sealer in the prepared canal space. The method for evaluating obturation quality in this study allowed for a direct observation of the amount of solid core versus the total area of prepared canal17).
It is concluded therefore that, under the conditions of the present study, the non-standardized size medium gutta-percha cone resulted in more efficient obturation than the ISO-standardized master gutta-percha cone as a master cone when lateral compaction technique was used in curved canals prepared with 0.06 tapered nickel-titanium rotary instruments.
Further investigation is needed on the obturation effect of these taper master cones in extracted teeth and on the long-term prognosis in patients.



 XML Download
XML Download