

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. INTRODUCTION
Dental resin composite shrinks by 1 - 5vol% during polymerization. Due to the polymerization shrinkage, clinical problems such as postoperative sensitivity, secondary caries, and cracks can occur1-3). In addition, microcracks in the composite body can occur which lead to higher wear of the composite4).
The influence of polymerization shrinkage on cavities can be affected by restoration size, cavity configuration, placement technique and curing mode5-11). It has been reported that placing composite in Class II cavities leads to inward deformation of the cusps and the amount of deformation has been observed to vary from 15 to 50 µm12).
Although it is accepted that polymerization shrinkage of the composite induces cuspal deflection, it is not yet clear whether variation occurs among materials or varying degrees of polymerization, polymerization shrinkage stress and modulus of elasticity. Lee & Park (2004)13) reported that there was no correlation between polymerization shrinkage stress and cuspal deflection of teeth. There was also no correlation found between the amount of linear polymerization shrinkage and shrinkage stress14).
The purpose of the present study was to evaluate the relationship between amount of polymerization shrinkage and cuspal deflection. A null hypothesis is there is no correlation between them.
II. MATERIALS AND METHODS
A. Linear shrinkage measurement
Six brands of light cured composites and two brands of polyacid modified resin composite were used (Table 1). Specimens were transferred to a Teflon mold to ensure that the same amount of composite and polyacid modified resin composite was used for each linometer sample. Specimens were transferred to the disk in the custom-made linometer (R & B, Daejeon, Korea) which had been previously coated with a separating glycerin gel and then covered with a glass slide and loaded under constant pressure. The surface of the glass slide facing the specimen was also coated with the separating gel. Specimens were light cured with a quartz tungsten halogen curing unit (XL3000, 3M Dental Product, St. Paul, USA), with a power density of 730 mW/cm2 when measured with a Coltolux Light Meter (Coltene, Altstätten, Switzerland). The tip of the curing light was positioned 2 mm above the slide glass and specimens were light cured for 60s. As the composite under the slide glass was cured, it shrank toward the light source and the aluminum disk under the composite moved upward. The amount of disk displacement, which was caused by the linear shrinkage of the resin composite, was measured using an eddy current sensor. The digital data were recorded on a computer for 60s using Microsoft Excel 2002 program. Ten measurements were made for each group and the amount of linear shrinkage occurring in 60s was statistically compared by an one-way ANOVA test and we used a Tukey's test as a post hoc test at the 95% confidence level.
B. Cuspal deflection measurement
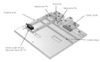
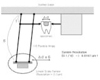
Recently extracted upper premolars which had no cracks, caries or any other defect were used. Special care was taken to control the tooth shape and size; bucco-lingual diameter, and crown height. Modified MOD cavities were prepared 3 mm deep, and 3.5 mm wide (Figure 1). After cleansing the cavity and tooth with fluoride-free pumice, a self-etching primer system (SE-bond, Kuraray, Okayama, Japan) was applied according to the manufacturer's instructions. The teeth were weighed. Using the Teflon mold, the same volume of composite or polyacid modified resin composite (Table 1) was measured and transferred to the cavities and bulk filled. Before and after the cavities were filled, the weight of the tooth specimens were also measured. The specimens were then positioned in the custom-made cuspal deflection measuring system (R & B Inc., Daejon, Korea) using the screw and pin. The point where the pin was positioned on the tooth surface was controlled through the specimens. When the specimens were positioned using the screw on one cusp tip, the pin, which was positioned in the other cusp tip, was pushed back. The change in the position of the pin was transferred to the floating lever and the movement of floating lever was detected by a Linear scale sensor (Lie5, Numerik Jena Gmbh, Jena, Germany). When the specimen was positioned, the intercuspal distance was set at zero point. The specimens were light cured from the occlusal, mesial and distal surface for 60s each. The inward cuspal movement changed the position of the pin and floating lever. As the degree of lever movement, where the pin was positioned, was multiplied 6 times at the other end of the lever arm, where the Linear scale sensor was positioned, the resolution of the sensor was increased by 6 times. Data were stored in computer simultaneously for 10 minutes (Figure 2 & 3). Fifteen specimens were used for each material. The amount of cusp movement was compared among materials by one-way ANOVA and Tukey's test at the 95% confidence level.
III. RESULTS
1. Measurement of linear polymerization shrinkage
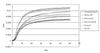
The average thickness of the samples was 1.60 ± 0.04. The amount of linear polymerization shrinkage is summarized in Table 2. The amount of linear polymerization shrinkage from least to greatest is Surefil, Heliomolar < Heliomolar HB < Synergy Compact, Z100 < Dyract AP < Pyramid, Compoglass F (p < 0.05), and ranged from 8.6 ± 4 µm to 10.9 ± 1 µm.
The pattern of linear polymerization shrinkage for the materials is shown in Figure 4. In all groups, the slope of curve is steep in the first 20s and thereafter it becomes more gradual.
2. Measurement of cuspal deflection
The amount of cuspal deflection is summarized in Table 3. The amount of cuspal deflection in ascending order is Z100, Heliomolar, Heliomolar HB, Synergy Compact, Surefil, < Compoglass F < Pyramid, Dyract (p < 0.05) and ranged from 14.63 ± 2.32 µm to 22.75 ± 3.36 µm.
The degree of cuspal deflection versus time is shown in Figure 5. In all groups, the slope of curve is steep in the first 300s and thereafter it becomes more gradual. In all groups, there is a slight jump in the slope in 180s.
3. Correlation between polymerization shrinkage amount versus cuspal deflection
The amount of the polymerization shrinkage and cuspal deflection were correlated (p < 0.001, Pearson Correlation Constant 0.54076) (Figure 6).
IV. DISCUSSION
The results of this study indicate that the amount of polymerization shrinkage and cuspal deflection were highly correlated. The materials that showed a lower shrinkage value also demonstrated lower cuspal deflection. As cuspal deflection increases, the chances of crack formation in a tooth would also increase and may also cause clinical symptoms such as temperature sensitivity and pain on biting. Therefore, in large class II cavities, resin composite with a low polymerization shrinkage value should be used to reduce cuspal deflection.
Lee and Park13) indicated that there were no correlation between amount of polymerization shrinkage stress and cuspal deflection. Even though one material has a low shrinkage value, it may have a high shrinkage stress depending on the modulus of elasticity of the material14). For example, in their study, Surefil, which showed the lowest shrinkage value in the present study was reported to have the highest shrinkage stress value when the same materials were compared for shrinkage stress value. The polymerization shrinkage stress of a material may have a greater effect on the marginal integrity of a cavosurface margin rather than cuspal deflection. It has been reported that polymerization shrinkage stress of composites has a different effect on the cavity depending on the configuration factor7). It was reported that leakage results correlated with stress values, i.e. composites with higher contraction stress showed more extensive marginal leakage.15). Whereas Lutz et al.11) reported that both quality and stress resistance of marginal adaptation were inversely correlated to intercuspal narrowing caused by the polymerization contraction of bonded and a well adapted resin restoration. According to their work, the most effective factors that can optimize marginal quality include: guidance of shrinkage vectors, reducing the ratio of bonded to free unbonded restoration surfaces, and minimizing the mass of in situ-cured composite. The relationship between amount of polymerization shrinkage, polymerization shrinkage stress, marginal adaptation needs further study.
In this study, most of the polymerization shrinkage of composites and polyacid modified resin composite occurred within the first 20s and reached a plateau even though a slight increase continued. This is consistent with the results of previous studies16,17). However, cuspal deflection was slower and longer than polymerization shrinkage of composites and compomers and reached a plateau between 300 - 500s. The remaining tooth structure seems to resist flexure in the early phase of the polymerization process. The time delay may be dependent on the remaining tooth structure, but it needs further investigation.
In the present study, modified MOD cavities, 3.5 mm wide and 3 mm deep, were prepared instead of conventional MOD cavities. This was to simplify and standardize the cavity design. As the amount of cuspal deflection was relatively small and we had to compare the data between materials, it was particularly important to minimize the variability and control error. A conventional MOD cavity is more complex in design and small variations in cavity preparation might have influenced the results of cuspal deflection. Therefore, a simpler cavity design was applied.
Abbas et al.18) reported that type of curing light (halogen or plasma arc curing) and curing method, bulk or incremental could affect the amount of cuspal deflection and microleakage. They reported that cuspal deflection was the highest, whereas the microleakage was lowest when the composites were incrementally cured using a halogen lamp. According to this study, bulk curing using a plasma arc lamp induced insufficient composite cure and resulted in lesser cuspal deflection and more leakage. In the present study, the composites were bulk cured for 180s (occlusal 60s, mesial 60s, distal 60s) using a halogen lamp. In the pilot of this study, we compared bulk and incremental curing methods for determining cuspal deflection. Even though there was no difference in the average between the two methods when the composite were sufficiently cured, there were more deviations in cuspal deflection data when incremental curing was used. The movement of cusps during composite manipulation with the incremental technique was considered to induce more deviations, therefore, bulk curing was used.
Heliomolar showed the lowest shrinkage value and was one of the materials which showed lowest inter-cuspal deflection. Park et al.14) and Lim et al.19) reported that it showed also the lowest shrinkage stress value. Some of the resin matrix in Heliomolar is in the form of prepolymerized particles that do not contribute to polymerization shrinkage. The characteristics of Heliomolar that have a low amount of shrinkage, low shrinkage stress and low cuspal deflection might be the reason for the long term clinical success of this material20).
Chung and Roh21) reported that SE Bond recorded higher bond strengths to tooth structure when different resin composites and bonding agents were compared. They also indicated that the combination of resin composite and dentin adhesive system recommended by the manufacturer did not always result in a positive effect. If sufficient bond strength was not produced, gaps may be formed between the filling material and tooth, that may influence cuspal deflection. This is the reason why the same bonding system (SE Bond) was used for the different restorative materials.
Table 4 shows the wt % of filler contents of the tested materials, which was provided by the manufacturers. When we compare the filler content of the materials in Table 4 and shrinkage data of present study, it can be seen that high filler content of a filling material does not always guarantee low polymerization shrinkage. The lower the initial viscosity of the material, the more monomer must be converted into polymer chains and networks. Although the space occupied by the filler particles does not participate in curing contraction, high filler loads require low molecular weight monomers to ensure proper handling viscosity. Within certain limits, polymerization shrinkage is not dependent on filler load. The lower molecular weight monomers in packable composites and polyacid modified resin composite which is added to control the handling viscosity may be responsible for the higher shrinkage value.
V. CONCLUSION
Most of the linear polymerization shrinkage occurred in the first 20s and the amount was different between materials. In cuspal deflection, it occurred more slowly than the polymerization shrinkage and the amount was different between materials. The amount of linear polymerization shrinkage and cuspal deflection were highly correlated and the null hypothesis was rejected.







 XML Download
XML Download