

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Objective
Authors conducted the pilot trial to evaluate whether the virtual reality using mirror therapy induces analgesia and functional improvement to the patients of rheumatoid wrist arthritis.
Method
Three patients with no symptom or sign of active phase at both wrists were recruited. Voluntary range of motion (ROM) of each wrist over as far as possible was recorded and then the same movement was recorded only over 60% of the previous one after break of 5 minutes. For the virtual reality treatment, the second recorded motion was reconstructed into the another one of as same ROM and spent time as the first one, providing confusing visual information to the patients while patients were instructed to reach only the red flags (60% ROM of 1st one). This exercise was repeated for 5 days. Numerous scales such as VAS, ROM, Michigan Hand Outcomes Questionaire (MHQ), Performance and Satisfaction in Activities of Daily Living (PS-ADL), patient-rated wrist evaluation (PRWE) were evaluated before and after repetition.
Figures and Tables
Fig. 1
Diagram of virtual reality. Patients were instructed to took a seat upright in a chair opposite to the table on which a monitor of virtual reality was placed, stretche their either of arm out into the support for the elbow, replace their wrist and hand in an anatomical neutral position under a camera to be seen fully in the center of the monitor, and their forearm and wrist were immobilized to the supports using Velcro strap.

Fig. 2
Preparation of virtual reality. Patients were instructed to grip a white poles using the palm surface so that the tip of the while pole was protruded beyond the ulnar border. Two red- colored round stickers of 1 cm in diameter were affixed to the center of wrist strap and the tip of the white pole respectively.

Fig. 3
Process of virtual reality. Patients were instructed to do flexion-extension wrist exercise again up- and down-ward to two red frags the location of which in a monitor was seen as the same as during the former exercise of full range. But virtual reality let the real-time movement of the wrist (white spot; 60% of previous range of motion) be seen to reach to the red flag in the pace of the same angular velocity.

Table 1
Interval Changes of Functional and Surrogate Ends
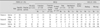
( ); normal range of corresponding scale.
The improved satisfaction with each hand or ADL was noticed after the virtual reality treatment for 5 days. Interval changes in others were variable. PRWE: patient-rated wrist evaluation, PS-ADL: performance & satisfaction in activities of daily living, MHQ: Michigan Hand Outcomes Questionnaire.
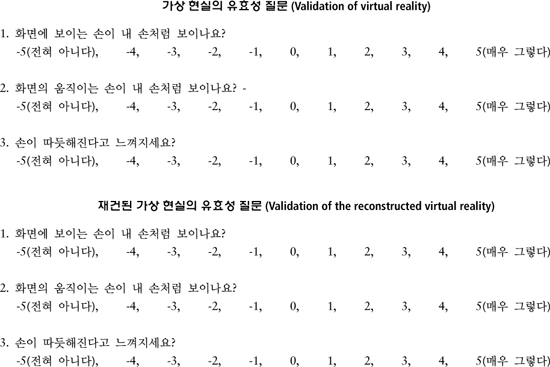
Table 2
Validity of the Virtual Reality

References
1. Ramachandran VS, Rogers-Ramachandran D. Synaesthesia in phantom limbs induced with mirrors. Proc Biol Sci. 1996; 263:377–386.

2. Ramachandran VS, Altschuler EL. The use of visual feedback, in particular mirror visual feedback, in restoring brain function. Brain. 2009; 132:1693–1710.
3. Moseley GL. Using visual illusion to reduce at-level neuropathic pain in paraplegia. Pain. 2007; 130:294–298.
4. Karmarkar A, Lieberman I. Mirror box therapy for complex regional pain syndrome. Anaesthesia. 2006; 61:412–413.
5. Ramachandran VS, Seckel EL. Using mirror visual feedback and virtual reality to treat fibromyalgia. Med Hypotheses. 2010; 75:495–496.
6. Yavuzer G, Selles R, Sezer N, Sutbeyaz S, Bussmann JB, Koseoglu F. Mirror therapy improves hand function in subacute stroke: a randomized controlled trial. Arch Phys Med Rehabil. 2008; 89:393–398.
7. Lee HM, Li PC, Fan SC. Delayed mirror visual feedback presented using a novel mirror therapy system enhances cortical activation in healthy adults. J Neuroeng Rehabil. 2015; 12:56.
8. Waljee JF, Chung KC, Kim HM, Burns PB, Burke FD, Wilgis EF. Validity and responsiveness of the Michigan Hand Questionnaire in patients with rheumatoid arthritis: a multicenter, international study. Arthritis Care Res (Hoboken). 2010; 62:1569–1577.
9. Holmes NP, Crozier G, Spence C. When mirrors lie: visual capture of arm position impairs reaching performance. Cogn Affect Behav Neurosci. 2004; 4:193–200.
10. Romano D, Bottini G, Maravita A. Perceptual effects of the mirror box training in normal subjects. Restor Neurol Neurosci. 2013; 31(4):373–386.
11. Chung KC, Pillsbury MS, Walters MR, Hayward RA. Reliability and validity testing of the Michigan Hand Outcomes Questionnaire. J Hand Surg Am. 1998; 23:575–587.
12. Archenholtz B, Dellhag B. Validity and reliability of the instrument Performance and Satisfaction in Activities of Daily Living (PS-ADL) and its clinical applicability to adults with rheumatoid arthritis. Scand J Occup Ther. 2008; 15:13–22.
13. MacDermid JC, Turgeon T, Richards RS, Beadle M, Roth JH. Patient rating of wrist pain and disability: a reliable and valid measurement tool. J Orthop Trauma. 1998; 12:577–586.
14. Norkin C WJ. Measurement of joint motion: a guide to goniometry. Philadelphia, PA: Davis Company;1995. p. 89–90.
15. Darnall BD, Li H. Home-based self-delivered mirror therapy for phantom pain: a pilot study. J Rehabil Med. 2012; 44:254–260.
16. Botvinick M, Cohen J. Rubber hands feel touch that eyes see. Nature. 1998; 391:756.
17. Garry MI, Loftus A, Summers JJ. Mirror, mirror on the wall: viewing a mirror reflection of unilateral hand movements facilitates ipsilateral M1 excitability. Exp Brain Res. 2005; 163:118–122.
18. Harris AJ. Cortical origin of pathological pain. Lancet. 1999; 354:1464–1466.
19. Flor H, Elbert T, Knecht S, Wienbruch C, Pantev C, Birbaumer N. Phantom-limb pain as a perceptual correlate of cortical reorganization following arm amputation. Nature. 1995; 375:482–484.
20. Flor H, Denke C, Schaefer M, Grusser S. Effect of sensory discrimination training on cortical reorganisation and phantom limb pain. Lancet. 2001; 357:1763–1764.
21. Maihofner C, Handwerker HO, Neundorfer B, Birklein F. Cortical reorganization during recovery from complex regional pain syndrome. Neurology. 2004; 63:693–701.
22. Pleger B, Tegenthoff M, Ragert P, Forster AF, Dinse HR, Schwenkreis P. Sensorimotor retuning [corrected] in complex regional pain syndrome parallels pain reduction. Ann Neurol. 2005; 57:425–429.
23. Kolb B, Whishaw IQ. Brain plasticity and behavior. Annu Rev Psychol. 1998; 49:43–64.
24. Funase K, Tabira T, Higashi T, Liang N, Kasai T. Increased corticospinal excitability during direct observation of self-movement and indirect observation with a mirror box. Neurosci Lett. 2007; 419:108–112.
25. Touzalin-Chretien P, Ehrler S, Dufour A. Dominance of vision over proprioception on motor programming: evidence from ERP. Cereb Cortex. 2010; 20:2007–2016.
26. Schaefer M, Flor H, Heinze HJ, Rotte M. Morphing the body: illusory feeling of an elongated arm affects somatosensory homunculus. Neuroimage. 2007; 36:700–705.
27. Schaefer M, Heinze HJ, Rotte M. My third arm: shifts in topography of the somatosensory homunculus predict feeling of an artificial supernumerary arm. Hum Brain Mapp. 2009; 30:1413–1420.
28. Egsgaard LL, Petrini L, Christoffersen G, Arendt-Nielsen L. Cortical responses to the mirror box illusion: a high-resolution EEG study. Exp Brain Res. 2011; 215:345–357.
29. Liepert J, Miltner WH, Bauder H, Sommer M, Dettmers C, Taub E. Motor cortex plasticity during constraint-induced movement therapy in stroke patients. Neurosci Lett. 1998; 250:5–8.
30. Kang YJ, Ku J, Han K, Kim SI, Yu TW, Lee JH. Development and clinical trial of virtual reality-based cognitive assessment in people with stroke: preliminary study. Cyberpsychol Behav. 2008; 11:329–339.
31. Keshavarz B, Hecht H. Validating an efficient method to quantify motion sickness. Hum Factors. 2011; 53:415–426.
 XML Download
XML Download