

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Objective
The aim of this study was to evaluate the relationship between motor evoked potentials (MEPs) or somatosensory evoked potentials (SSEPs) and the recovery of function in acute or subacute stroke patients.
Method
Twenty one hemiplegic stroke patients were examined with MEPs of extensor carpi radialis, abductor pollicis brevis, tibialis anterior and abductor hallucis and SSEPs of median and tibial nerves. A separate score was defined for upper and lower extremities within the Fugl-Meyer assessment and Korean-modified Barthel index. Motor performances were evaluated simultaneously with the evoked potential assessments and at 2 weeks after the first examination.
Results
The second motor function of upper extremity was significantly higher in patients with the presence of MEP or SSEP (p<0.05). The improvement of self care was correlated with the responsiveness in SSEP. Motor function of lower extremity was significantly associated with the responsiveness in MEP or SSEP (p>0.05). MEP in tibialis anterior or tibial SSEP were correlated with the mobility.
Figures and Tables
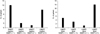 | Fig. 1Distribution of patients according to presence of MEP and SSEP. FMU: Fugl-Meyer score of upper extremity, FML: Fugl-Meyer score of lower extremity, UMEP: MEP in upper extremity, LMEP: MEP in lower extremity, (+): Response, (-): No response.
|
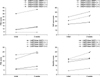 | Fig. 2Changes in FMA subscores and K-MBI subscores according to presence of MEP and SSEP in upper and lower extremities. *p<0.05, p-value was derived from Wilcoxon signed ranks test. FMU: Fugl-Meyer score of upper extremity, FML: Fugl-Meyer score of lower extremity, UMEP: MEP in upper extremity, LMEP: MEP in lower extremity, (+): Response, (-): No response.
|

Table 2
Relationships Between Upper-Extremity Evoked Potentials and Occurrence of Motor and Functional Recovery

Values are mean ± standard deviation. EP: Evoked potential, MEPs: Motor evoked potentials, SSEPs: Somatosensory evoked potentials, FMU: Fugl-Meyer score of upper extremity, ECR: Extensor carpi radialis, APB: Abductor pollicis brevis *p<0.05, p-value was derived from Mann-Whitney U test. †p<0.05, p-value was derived from Wilcoxon signed ranks test.
![]()
Table 3
Relationships Between Lower-Extremity Evoked Potentials and Occurrence of Motor and Functional Recovery

Values are mean ± standard deviation. EP: Evoked potential, MEPs: Motor evoked potentials, SSEP: Somatosensory evoked potentials, FML: Fugl-Meyer score of lower extremity, TA: Tibialis anterior, AH: Abductor hallucis. *p<0.05, p-value was derived from Mann-Whitney U test. †p<0.05, p-value was derived from Wilcoxon signed ranks test.
![]()
References
1. Escudero JV, Sancho J, Bautista D, Escudero M, Lopez-Trigo J. Prognostic value of motor evoked potential obtained by transcranial magnetic brain stimulation in motor function recovery in patients with acute ischemic stroke. Stroke. 1998. 29:1854–1859.
2. Rapisarda G, Bastings E, de Noordhout AM, Pennisi G, Delwaide PJ. Can motor recovery in stroke patients be predicted by early transcranial magnetic stimulation? Stroke. 1996. 27:2191–2196.
3. Heald A, Bates D, Cartlidge NEF, French JM, Miller S. Longitudinal study of central motor conduction time following stroke, 2: central motor conduction measured within 72h after stroke as a predictor of functional outcome at 12 months. Brain. 1993. 116:1371–1385.
4. Kang MJ, Yoon TS, Park CI, Chun SI. Motor Evoked Potential in Stroke. J Korean Acad Rehabil Med. 1993. 17:26–35.
5. Kang DW, Park SH, Lee YJ, Chun JU, Ko SB, Yoon BW, Lee KW, Roh JK. Early Transcranial Magnetic Stimulation Can Predict Motor Recovery of Subacute Stage in Acute Ischemic Stroke Patients. Korean J Stroke. 2000. 2:57–61.
6. Kim C, Jeong J. The Significance of Motor Evoked Potentials as a Prognostic Factor in the Early Stage of Stroke Patients. J Korean Acad Rehabil Med. 1999. 23:1213–1220.
7. Han TR, Bang MS, Lee KW. Motor evoked potentials of upper and lower extremities by magnetic stimulation in hemiparesis. J Korean Acad Rehabil Med. 1998. 22:386–391.
8. Jung HY, Kim TH, Park JH. Relationship of national institute of health stroke scale and motor evoked potentials in subjects with stroke. J Korean Acad Rehabil Med. 2005. 29:563–567.
9. Rossini PM, Barker AT, Berardelli A, Caramia MD, Caruso G, Cracco RQ, Dimitrijevic MR, Hallett M, Katayama Y, Lucking CH, Noordhout MD, Marsden CD, Murray NMF, Rothwell JC, Swah M, Tomberg C. Non-invasive electrical and magnetic stimulation of the brain, spinal cord and roots: basic principles and procedures for routine clinical application. Report of an IFCN committee. Electroencephalogr Clin Neurophysiol. 1994. 91:79–92.
10. Turton A, Wroe S, Trepte N, Fraser C, Lemon C. Contralateral and ipsilateral EMG responses to transcranial magnetic stimulation during recovery of arm and hand function after stroke. Electroencephalogr Clin Neurophysiol. 1996. 101:316–328.
11. Colebatch JG, Gandevia SC. The distribution of muscular weakness in upper motor neuron lesions affecting the arm. Brain. 1989. 112:749–763.
12. Thorsen RA, Occhi E, Boccardi S, Ferrarin M. Functional electrical stimulation reinforced tenodesis effect controlled by myoelectric activity from wrist extensors. J Rehabil Res Dev. 2006. 43:247–256.
13. Lee RG, van Donkelaar P. Mechanisms underlying functional recovery following stroke. Can J Neurol Sci. 1995. 22:257–263.
14. Allen CMC. Predicting the outcome of acute stroke: a prognostic score. J Neurol Neurosurg Psychiatry. 1984. 47:475–480.
15. Anderson TP. Studies up to 1980 on stroke rehabilitation outcomes. Stroke. 1990. 21:1143–1145.
16. Zeman BD, Yiannikas C. Functional prognosis in stroke: use of somatosensory evoked potentials. J Neurol Neurosurg Psychiatry. 1989. 52:242–247.
17. La Joie WJ, Reddy NM, Melvin JL. Somatosensory evoked potentials: their predictive value in right hemiplegia. Arch Phys Med Rehabil. 1982. 63:223–226.
18. Barker AT. An introduction to the basic principles of magnetic nerve stimulation. J Clin Neurophysiol. 1991. 8:26–37.
19. D'Olhaberriague L, Gamissans JME, Marrugat J, Valls A, Oliveras Ley C, Seoane JL. Transcranial magnetic stimulation as a prognostic tool in stroke. J Neurol Sci. 1997. 147:73–80.
20. Macdonell RAL, Donnan GA, Bladin PF. A comparison of somatosensory evoked and motor evoked potentials in stroke. Ann Neurol. 1989. 25:68–73.
21. Fugl-Meyer AR, Jääskö L, Leyman I, Olesson S, Steqlind S. The post-stroke hemiplegic patient, I: a method for evaluation of physical performance. Scand J Rehabil Med. 1975. 7:13–31.
22. Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md State Med J. 1965. 14:61–65.
23. Shah S, Vanclay F, Cooper B. Improving the sensitivity of the barthel index for stroke rehabilitation. J Clin Epidemiol. 1989. 42:703–709.
24. Jung HY, Park BK, Shin HS, Kang YK, Pyun SB, Paik NJ, Kim SH, Kim TH, Han TR. Development of the Korean Version of Modified Barthel Index (K-MBI): Multi-center Study for Subjects with Stroke. J Korean Acad Rehabil Med. 2007. 31:283–297.
25. Warabi T, Inoue K, Noda H, Murakami S. Recovery of voluntary movement in hemiplegic patients. Correlation with degenerative shrinkage of the cerebral peduncles in CT images. Brain. 1990. 113:177–189.
26. Kim JH, Han TR, Lee SJ. The posterior tibial nerve somatosensory evoked potentials in the hemiplegic patients. J Korean Acad Rehabil Med. 1993. 17:525–533.
27. Hendricks HT, Pasman JW, van Limbeek J, Zwarts MJ. Motor evoked potentials of the lower extremity in predicting motor recovery and ambulation after stroke: a cohort study. Arch Phys Med Rehabil. 2003. 84:1373–1379.
28. Dobkin BH, Firestine A, West M, Saremi K, Woods R. Ankle dorsiflexion as an fMRI paradigm to assay motor control for walking during rehabilitation. Neuroimage. 2004. 23:370–381.
29. Perry J. Gait analysis: Normal and Pathologic Function. 1992. Thorofare, NJ: SLACK Inc;55–57.
30. Kwon JY, Kim JS, Park SW, Jang SJ, Kim BS. Influence of Aphasia on the Cognitive Screening Test in Stroke Patients with Unilateral Cerebral Hemispheric Lesion. J Korean Acad Rehabil Med. 2002. 26:9–13.
31. Han TR, Kim JH, Lim JY. Proper facilitation technique for bilateral motor evoked potentials by transcranial magnetic stimulation. J Korean Acad Rehabil Med. 2000. 24:65–71.
 XML Download
XML Download