

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Spondylolysis involves a defect of the pars interarticularis1. The pars interarticularis is a small isthmus of bone between the superior and inferior articular facets of a spinal vertebra. This defect can occur at any level, but is most commonly seen in the lumbar spine, particularly at the L5 level (85%–95%)2. Low back pain (LBP) is a common symptom in young competitive athletes and a frequent reason for lost training and playing time. Chronic severe LBP in young athletes may be caused by spondylolysis3. Although spondylolysis also may be found in the cervical spine45, it is rarely seen in the upper lumbar region. In addition, we are not aware of any published reports on consecutive levels of spondylolysis occurring several years later. Here, we describe a case of consecutive spondylolysis at the L3 and L4 levels in an elite soccer player, underscoring the possibility of consecutive levels of spondylolysis resulting from certain sports.
Case Report
1. History
A 26-year-old male elite soccer player was referred to Incheon Himchan Hospital for severe LBP. Written informed consents were obtained. There was no definitive traumatic episode, but he underwent 2 weeks of conservative treatment for spondylolysis at the L3 level. He felt back pain when he did hyperextension movement, but pain was not aggravated other exercises and relieved after rest. Two years later, he again experienced severe LBP, exacerbated by extension of his back while playing soccer. After 3 weeks of experiencing LBP, he was referred to our outpatient clinic.
2. Examinations
Neurologic examination showed no abnormal findings. Physical examination demonstrated normal gait and alignment of the spine and pelvis. He experienced no difficulty during flexion, but felt discomfort during extension of the spine. Tenderness could be elicited at the paraspinal muscle area and spinous processes of the lower lumbar spine.
3. Radiologic findings
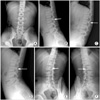
In 2014, plain radiography of the lumbar spine showed no obvious abnormalities except for mild scoliosis with slight left rotational deformity at the L3 level (Fig. 1A). On lateral imaging, a disconnected line at the isthmus of the L3 vertebra could be seen (Fig. 1B). On dynamic imaging, bilateral disconnected lines at the pars interarticularis were seen without instability (Fig. 1C–F). In 2016, plain anteroposterior imaging showed no abnormalities or scoliosis. Lateral radiography of the lumbar spine showed a fracture line at L3 and L4 (Fig. 2A). Dynamic flexion-extension imaging showed a disconnected line at the isthmus of L3 and L4 (Fig. 2B, C), while oblique imaging showed a fracture line. It was typical sign of hyperextension injuries on radiography. The initial diagnosis in 2014 was L3 spondylolysis, whereas the final diagnosis in 2016 was stress fracture of both interior articular processes (early-stage spondylolysis) of the L3 and L4 vertebrae. Computed tomography showed a discontinued line at the pars interarticularis (Fig. 2D). Magnetic resonance imaging confirmed a discontinued line at the pars interarticularis of L3 and L4. Hypertrophied foraminal ligament suspected repetitive trauma of L4 intervertebral foramen after L3 fracture. L4 also showed T2 weighed low signal intensity suggesting subacute or late fracture healing (Fig. 2E, F).
4. Treatment
As he was a member of a professional soccer team, he could not undergo long-term bracing or take sick leave. Long-term bracing may cause rigid spine, impeding performance. Hence, exercise was stopped for 3 months, with further stretching of the hip joint and other levels of the lumbar spine.
Discussion
Spondylolysis is thought to result from repeated stress on the spine, but most cases involve only a single lumbar lesion. More than 90% of patients have spondylolysis at the most caudal level (L5) as a pars interarticularis defect3, while fewer patients have spondylolysis in the cervical spine45. Spondylolysis has been reported to occur in approximately 6% of the general population and twice as often in men than in women. Micheli and Wood6 reported that after examining 100 adolescents with LBP, 47 (47%) had spondylolysis. This finding contradicts the 6% of adults with LBP who are found to have spondylolysis. Donaldson7 reported nine seasons of ice hockey, during which 25 players complained of LBP. Among them, 44% had spondylolysis. They concluded that spondylolysis is very common in adolescents, but somewhat rare in adults, and that specific diagnostics should not be delayed, as serious harm can occur. A contributing factor as to why spondylolysis is more common in adolescents than in adults is that the spine is still undergoing growth and remodeling8. In fact, the pars interarticularis does not achieve bony maturity until approximately age 25.
Adolescent athletes with persistent LBP that worsens with extension should be suspected as having spondylolysis and referred for further diagnostic testing to rule out spondylolysis and/or spondylolisthesis6. Diagnostic testing will most often begin with radiography. The best angle for viewing the pars interarticularis is the lateral oblique view89. However, this view may not adequately show early, newly developing spondylolysis. Further imaging studies may include single-photon emission computed tomography, computed tomography, and/or magnetic resonance imaging.
There is no consensus on the most effective interventions for spondylolysis. One frequently used intervention is rest from sports and exercise. Our case also as a soccer player usually complained back pain on hyperextension exercise and relieved when he took a rest. Several studies have suggested that individuals rest from sports for at least 3 months8; however, the amount of rest can vary from 2 weeks to 6 months, depending on the severity of symptoms and the goal of the intervention. Some authors have reported that their goal is to achieve stable, pain-free union of the pars interarticularis fracture1, whereas others have reported a goal of pain-free motion and return to full activity, without necessarily attaining complete bony healing9. One commonly used intervention for adolescent athletes is bracing of the lumbar spine8. Many authors recommend that individuals wear the brace for 24 hours a day. Sairyo et al.10 recommended a soft brace for both the lumbar and thoracic spines.
It may be difficult to diagnose spondylolysis because of its rarity. In the present case, lateral radiographs showed deficits similar to those observed in early lumbar spondylosis at consecutive levels. To the best of our knowledge, no previous report has described consecutive levels of spondylolysis including stress fracture. Athletes may present with unusual spinal injuries, such as lumbar spondylolysis, which reflect stressors specific to their sport.

 XML Download
XML Download