

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In medical care, treatment has traditionally been performed following tests and diagnosis based on objective medical indicators such as biochemical tests, physiological tests, and imaging tests. However, in “treatment evaluation”, subjective health outcomes of patients are considered essential as medical indicators. The concept of patient-reported outcomes (PRO) is currently spreading and being used to evaluate patients' subjective quality of life (QOL). In the field of oral health, the Oral Health Impact Profile (OHIP)1 is used as a QOL scale with verified reliability and validity.2 In addition, the General Oral Health Assessment Index (GOHAI)3 is used as an oral health-related QOL scale with reported national standard scores for Japanese people.45 Previous research involving PRO has indicated an association between the number of remaining teeth and tongue pain as a factor affecting the oral health-related QOL in elderly people living in rural areas.6 Another report stated that oral healthrelated QOL decreases regardless of age or sex when deterioration of the oral health status occurs, such as difficulty in eating or pain.7 In another study, PRO was used to evaluate the effect of prosthodontic treatment.8 Although studies related to implant treatment have been performed in other countries,91011 few studies involve Japanese. Thus, the aim of this study was to use PRO to evaluate oral health status and implant treatment in Japanese patients with missing teeth.
MATERIALS AND METHODS
This was a cross-sectional study. Subjects were patients who visited the Department of Oral Implantology at Osaka Dental University from 1 October 2014 to 31 March 2015. Of these patients, 804 who provided consent to participate in this study were subjected to analysis. The QOL scale used in this study was the standard Japanese version of GOHAI.4 GOHAI is widely used throughout the world and measures the degree of restriction of daily living caused by oral health-related problems from physical, psychological, and social aspects. The 12 questions are rated on a five-point scale (total score ranging from 12 to 60), and a higher score indicates a higher QOL.
The survey items included background data (age, sex, survey period, pre- or post-treatment), Eichner classification, and GOHAI score. The questionnaires were self-administered, distributed to, and collected from participants in a waiting room. For patients who were unable to understand the questionnaire content, the questions were read out slowly and carefully so as not to make interpretations that would produce a bias in the answers. To avoid survey overlap, multiple investigators checked the surveys following data input. The survey periods in this study were used to categorize patients who responded before prosthodontic treatment into an occlusal support loss group (pre-implant group) and patients for whom at least 6 months had passed since implant treatment and fitting of a superstructure into an occlusal support restoration group (post-implant group). The 10 classifications of the Eichner Index (Al, A2, A3, B1, B2, B3, B4, C1, C2, and C3) ranked occlusion from ideal to non-existent. In the Eichner classification, each posterior contact area (premolar and molar) is counted as one region, for a total of four supporting zones. All “A” scores refer to occlusal contacts in all four premolar and molar regions; “Al” has all contacts, “A2” has missing teeth in one arch, and “A3” has missing teeth in both arches. All “B” scores refer to contacts in 0-3 posterior regions; “Bl” has three supporting zones, “B2” has two supporting zones, “B3” has one supporting zone, and “B4” has no opposing molar zone, with opposing contacts only in the anterior area. No “C” scores have opposing contacts; “Cl” scores have teeth in both arches that are not in contact; “C2” scores indicate teeth in one arch, while “C3” indicates that the subject is edentulous. Eichner classifications were determined by two dentists with reference to panoramic X-rays. Thereafter, patients classified as A1, A2, and A3 were assigned to a four-support group; B1 to a three-support group; B2 to a two-support group; B3 to a one-support group; and B4, C1, C2, and C3 to a zero-support group. The total score of all 12 questions on the GOHAI questionnaire was analyzed.
Exclusion criteria for survey participants were (1) missing background data, (2) missing data for more than half of the GOHAI questionnaire, (3) no panoramic X-rays performed, and (4) a combination of bridges, removable partial dentures, and implants in the oral cavity. In the post-implant group, an additional criterion of (5) a chief complaint other than missing teeth (diseases affecting QOL) was set.
The GOHAI scores were analyzed as follows: (1) the Kruskal-Wallis test was used to compare by number of occlusal supports in each group; and (2) Mann-Whitney's U test was used to compare the number of occlusal supports in both groups. The effect size (r), which indicates the strength of the relationship between variables, was also calculated.12 The level of statistical significance was set at less than 5%. All analysis was conducted using R version 3.1.0 (R Core Team, 2014. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria, http://www.R-project.org/). This study was conducted with the approval of the Ethics Committee of Osaka Dental University (approval number: 110786). In addition, GOHAI was used after submitting an application to iHope International (https://www.sf-36.jp/index.html) and receiving approval for its use.
RESULTS
Of the 804 participants, 377 were assigned to the preimplant group (median age: 60 years, range: 15 – 88 years) and 427 were assigned to the post-implant group (median age: 65 years, range: 20 – 88 years). The backgrounds of the participants classified according to the number of occlusal supports provided by the remaining teeth are presented in Table 1. In the pre-implant group, significant differences were observed in the ratios of sex and age. In the postimplant group, a significant difference was observed only in age (Table 1).
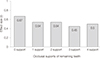
The GOHAI scores (median) based on the number of occlusal supports in the pre-implant group were 41.0 for zero supports, 42.0 for one support, 46.0 for two supports, 46.5 for three supports, and 47.0 for four supports. The results of multiple comparisons revealed a significant difference in GOHAI scores between zero and two supports, zero and three supports, zero and four supports, and one and four supports. GOHAI scores increased as the number of occlusal supports increased (P < .001). However, GOHAI scores in the post-implant group were 56.0 for zero supports, 53.0 for one support, 55.0 for two supports, 55.0 for three supports, and 56.0 for four supports. The results of the Kruskal-Wallis test revealed no significant differences in GOHAI scores on the basis of the number of occlusal supports in the post-implant group (Fig. 1).
Significant differences in GOHAI scores were observed between the pre-implant group and the post-implant group for all numbers of occlusal supports (P < .001), with GOHAI scores being higher in the post-implant group (Fig. 2). The effect size was 0.67 for zero supports, 0.54 for one support, 0.54 for two supports, 0.45 for three supports, and 0.50 for four supports (Fig. 3).
DISCUSSION
Average life expectancy has been increasing in Japan since the end of the Second World War, largely as a result of improvements in the living environment and advancements in medical technology. It is important for Japan's aging population to maintain function to continue enjoying a social life for as long as possible. Therefore, the extension of healthy life expectancy is cited as a guideline in Japan's health policy [Ministry of Health, Labour, and Welfare (MHLW), Healthy Japan 21 - Second Phase 2013]. At the “Healthy Japan 21” deliberation council (MHLW White Paper 2014), five indicators were presented: (1) the extension of healthy life expectancy and reduction of health disparities; (2) full prevention of the onset and aggravation of major lifestyle-related diseases; (3) the maintenance and improvement of functions necessary to continue having a social life; (4) the improvement of social environments to support and protect health; and (5) the improvement of living habits and social environments in relation to nutrition and diet, physical activity and exercise, relaxation, drinking, smoking, and dental and oral health. Oral function is associated with all these indicators, and a focus is being placed on the relationship between health maintenance/promotion and oral health.13 Previous studies have reported that a reduction in the number of teeth affects vital prognoses,14 and that people with masticatory function live longer.15 It has also been reported that the risk of heart disease increases when a person has few remaining teeth,14 that elderly people with few remaining teeth or mastication problems are more likely to require a higher level of nursing care,1617 and that the risk of dementia increases when a person has few teeth.18 The number of remaining teeth is therefore an important factor in the maintenance of oral function. In Japan, the 2011 Survey of Dental Diseases revealed that the proportion of people with 20 teeth was 25.1% in those aged 80 years, 47.6% in those aged 75 – 79 years, 52.3% in those aged 70 – 74 years, 69.6% in those aged 65 – 69 years, and 78.4% in those aged 60 – 64 years (MHLW 2011). It is thus conceivable that many elderly people are still undergoing prosthodontic treatment for tooth loss. Many patients are treated with removable partial dentures; however, it was difficult to objectively evaluate the intention (“it is difficult to talk” and “I am unwilling to use dentures”).
Nonetheless, many recent reports have used PRO in the evaluation of oral health status.1920 Hugo et al.21 found that QOL was lower in elderly edentulous patients who had been wearing complete dentures for a long time than in those who had been wearing dentures for less than 6 months for reasons such as poor retention. Furthermore, Nogawa et al.22 noted that in addition to the factor of the number of remaining teeth, the maintenance of oral function through appropriate oral management is important for improving QOL. However, patients struggle to form a specific picture of the significance of the QOL score, and patients in poor health find QOL surveys to be a burden or are prone to information bias when completing such surveys.23 Moreover, Fukuda23 evaluated QOL with the belief that “taking QOL surveys” does not always mean that “a patient's QOL is valued”. It is also conceivable that not performing prosthodontic treatment to replace missing teeth is sometimes better for increasing patient QOL because of the “hassle of hospital visits and treatment”. However, the choice not to perform prosthodontic treatment is not ideal for patients from the standpoint of protecting the remaining teeth. Limitations therefore exist in discussing the necessity of treatment based only on QOL evaluation. Nonetheless, QOL is considered to be an important indicator of therapeutic effects in the promotion of medical care based on evidence-based medicine. This study was therefore designed to use PRO to evaluate the oral health status and implant treatment of Japanese patients with missing teeth.
In this study, significant differences were observed in the ratios of sex and age within the pre-implant group and in age only within the post-implant group. Furthermore, most participants were aged between 50 and 70 years. The mean Japanese national standard GOHAI score of people in their 50 seconds is 53.1 [standard deviation (SD): ± 7.7, median: 56.5 (interquartile range: 47.0 – 60.0)] in men and 51.3 (SD: ± 7.9, median: 56.0; range: 46.0 – 58.0) in women. The mean Japanese national standard GOHAI score of people in their 60 seconds is 52.8 (SD: ± 7.4, median: 56.0; range: 47.0 – 59.0) in men and 52.4 (SD: ± 7.1, median: 54.0; range: 47.0 – 59.0) in women.4 These scores for both age ranges and sexes are similar, which suggests that neither was a confounding factor in this study. Moreover, the mean number of missing teeth per person in their 60 seconds in the 2011 Survey of Dental Diseases was found to be approximately six, which indicates that the participants in this study with zero or one occlusal support have more missing teeth than others of the same age and a lower GOHAI score than the national standard.11
GOHAI scores in the pre-implant group tended to be low when participants had few occlusal supports, and the scores were lower than the national standard for those of the same age for all numbers of occlusal supports. The interquartile range for zero supports in the pre-implant group was particularly small. This is because most participants in the zerosupport group did not record high GOHAI scores, despite a fixed rate of participants having high GOHAI scores in other occlusal support groups. This is consistent with reports that found a connection between a low number of remaining teeth plus dissatisfaction with masticatory ability and reduced QOL.212224 Elderly people often cite food as something they enjoy in daily life.25 The participants in this study were aged over 60 years, and the successful restoration of masticatory function in the post-implant group may have led to higher scores in terms of QOL. However, some participants in the pre-implant group with zero supports exhibited GOHAI scores of 50 or higher, and some participants with one support attained the maximum score of 60. This is inconsistent with the aforementioned reports that state that QOL is low when there are few occlusal supports. The subjects of this survey were patients who underwent examinations in the hope of receiving prosthodontic treatment for tooth loss. Nonetheless, it is possible that tooth loss has no effect on the GOHAI score or that the GOHAI scale itself causes a ceiling effect.
Furthermore, the post-implant group also exhibited higher GOHAI scores than the pre-implant group. Regardless of the number of occlusal supports, the post-implant group had higher QOL and scores similar to the national standard of those of the same age. The level of QOL achieved was similar to that of people in their 60 seconds in the Survey of Dental Diseases, who had a mean current number of approximately 22 teeth and occlusal support restored through implant treatment. Mastication difficulties, including “appetite” and “difficulty chewing” as noted by Hashimoto,26 are reportedly linked to reduced social satisfaction and day-to-day sense of health. Moreover, poor intraoral health results in continued dietary bias, which can be a cause of systemic diseases such as diabetes and heart disease. However, a limitation in this study is the inability to determine the areas in which the QOL summary scales, such as “restoration of esthetics” and “restoration of masticatory efficiency”, were high in the post-implant group. The participants in this survey were patients who were sufficiently healthy to be able to visit a university hospital. The fact that patients who were not healthy enough to visit the hospital were excluded from this study is thus another limitation.



 XML Download
XML Download