

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Caries is a common oral disease that progresses with the erosion of the hard tissue of a tooth by bacteria, and the erosion progresses from the outside of the tooth enamel to dentin. Among these, proximal caries occurs in the approximal surface between two teeth and the diagnosis with a visual examination or tactile sensation using a dental explorer may not be possible if a lesion is small.1 The progression of the lesion of proximal caries is fast, and its diagnosis is difficult among various sites of caries.2 Currently, the diagnostic methods for proximal caries generally in clinical use include visual inspection, tactile examination and radiography. According to previous studies, 75% of the proximal caries were found in the approximal surface, and 25% in the lower proximal surface.3 The proximal caries is normally discovered when the weakened marginal ridge is broken or a large cavity forms.4
Bitewing radiography is useful in the detection of proximal caries or secondary caries, the examination of the height of the ridge, and the determination of the existence of plaque.5 However, if the scanning line of X-ray does not exactly pass the approximal surface, the possibility of the superposition of structures is high, leading to the difficulty in detection.6 To address this issue, QLF-D (QLF-D Biluminator 2, Inspektor Research Systems BV, Amsterdam, Netherlands) and DIAGNOdent (DIAGNOdent Classic, KaVo Dental GmbH, Biberach, Germany) that can determine the severity of caries using fluorescence have been developed.
QLF is an equipment that can detect caries by irradiating teeth with the light in the blue visible wavelength range (405 nm).7 Its principle is to detect the red fluorescence generated by porphyrins that are metabolites of intraoral bacteria. Recently, QLF-D is equipped with an additional special filter (D007, Inspektor Research Systems BV) to show more accurate images. The sound tooth structure looks like actual tooth and caries lesion has red fluorescence in the current QLF-D.7 QLF-D can acquire both white light image and blue light image simultaneously. In addition, it can not only detect early caries or confirm the existence of plaque or tartar but also quantify the progression of caries since it shows the fluorescence loss in the lesion of caries numerically.8 Initial studies reported the high sensitivity and specificity of QLF-D, which were 0.67 and 0.70, respectively, for the detection of occlusal caries, and the quantified values were shown to have the high correlation coefficient of 0.82 with the caries lesion depth.9 Hence, QLF-D is a diagnostic tool with relatively well verified validity and reliability compared to other diagnostic equipment developed to date.8
DIAGNOdent irradiates a specific location of the tooth surface with laser of a 655 nm wavelength through optic fiber, and absorbs the infrared range fluorescence reflected from this specific site through optic fiber again, displaying its intensity numerically from 0 to 99. Hibst et al. initially suggested that the metabolites of bacteria in caries released fluorescence intensified by the laser.1011 DIAGNO dent can easily detect the caries lesion in the deep and narrow pit and fissure where an explorer normally cannot reach, and avoid the damage of enamel due to incorrect explorer maneuver on the early caries site. In general, this equipment has validity and reliability in detecting caries at the occlusal and approximal surfaces,12131415 and the outcome values have been known to be correlated with the extent of erosion.16 However, many prior studies showed that DIAGNOdent had low specificity despite high sensitivity since it could give false positives on foreign substance or restoration material in addition to the caries lesion.717
There are various prior studies on the detection of proximal caries using QLF-D to date, starting from the comparative study between QLF-D and DIAGNOdent on the quantification of smooth surface caries to a very recent comparative study on the diagnostic performance between International Caries Detection and Assessment Systems (ICDAS), QLF-D and digital radiography for the detection of proximal caries.1518 Also, regarding DIAGNOdent, of notable comparative studies are on the diagnostic performance between DIAGNOdent at the approximal surface, and DIAGNOdent and bitewing radiography at the nonapproximal surface for the detection of proximal caries of deciduous teeth, and the accuracy between DIAGNOdent and bitewing radiography for the detection of the same subject.13141920 However, there are few studies comparing all of QLF-D, DIAGNOdent, and bitewing radiography. The goal of this study was to examine the in vitro validity of QLF-D and DIAGNOdent with the diagnostic readings of digital bitewing radiography for the detection of proximal caries in extracted premolars.
MATERIALS AND METHODS
This study was conducted with 102 extracted human premolars without enamel hypoplasia or dental fluorosis selected from a pool of extracted permanent teeth at Department of Dentistry at Ewha Womans University Medical Center. This study was approved by the Institutional Review Board of Ewha Womans University and has been conducted in full accordance with the World Medical Association Declaration of Helsinki (Approval No: 2016-02-058). Among the subject teeth, those with severe destruction of crown, large restorations, and extensive caries involving more than half of the proximal surfaces were excluded based on the selection criteria of previously reported study.18 Extracted teeth were immediately immersed in distilled water to remove soft tissue and plaque completely, and stored at −20℃ until the assessment of caries. In order to simulate adjacent teeth in the oral cavity, the proximal surfaces and marginal ridges of two similar-shaped premolars were put into tight contact as pairs, and a total of 51 plaster blocks were fabricated. First of all, two teeth were arranged in the utility wax so that approximal surfaces could be in contact with each other, and then the index of crown part of teeth was taken with putty impression material (Extrude Xtra Putty, Kerr, Romulus, MI, USA). After the utility wax at the root of the tooth was removed, teeth were fixed in hard plaster (Neo Plumstone, Mutsumi Chemical Industry, Nigata, Japan) using the putty index.
In this study, three types of assessment methods for proximal caries were applied, which were bitewing radiography, QLF-D and DIAGNOdent. In order to eliminate interrater errors, all examinations were performed by a single skilled examiner who had sufficient training and practices of bitewing radiography, QLF-D and DIAGNOdent. The interpretation of radiographs obtained from bitewing radiography was performed by one calibrated dental professional specialized in radiology. In order to verify the intrarater reliability, all the examinations were performed twice with an interval of a week. For this, a week of the gap between the two examinations was decided on the ground that there would be no learning effect and at the same time, the skill of the examiner would not change.21 To assess proximal caries, bitewing radiography was performed using an intraoral X-ray equipment (CS 2100, Carestream Health, Trophy, France) and an intraoral digital sensor (RVG 6100, Carestream Health) with a customized holding jig. X-ray was taken under the constant condition of 60 kV, 7 mA, and 0.125 seconds of exposure time. In addition, the cone of the X-ray equipment was aligned by the customized jig to be at a distance of 4 cm from the specimen and 6 cm from the digital sensor for the standardized radiographs. In case of using QLF-D, fluorescence loss (ΔF) was measured to assess proximal caries. Before the examination, teeth were air-dried for 5 seconds, and then their images taken in three directions from buccal, occlusal and lingual surfaces using QLF-D in the dark room where all the lights were completely blocked. Images were taken under the constant condition using the specialized software (C3 v1.23, Inspektor Research Systems BV). The photographic conditions of QLF-D were as follows: shutter speed of 1/15 s, aperture value of 8.0, ISO speed of 1600, white balance as manual (white light) or daylight (blue light). The distance and angle between the sample and QLF-D were maintained to be 6 cm and 90°. The DIAGNOdent equipment has two liquid crystal displays, and one shows the actual value while the other shows the maximum value. The actual value means the currently measured real time value coming from the probe on the tooth surface, and the maximum value is the largest measured value thus far. In this study, after the Probe A was connected to DIAGNOdent, the largest value measured (maximum value) while the angle of the tip was changed in a circular movement was recorded as the representative value. The tip was fixed at the marginal ridge of occlusal surface and the interproximal space on the buccal and lingual side for each measurement.
For the analysis using bitewing radiography, the interpretation criteria of radiographs were set according to the study of Pitts,22 which classified the progress of caries to 4 stages (Table 1). If radiolucency was not observed at all on the radiography, it was classified as R0. If radiolucency was observed but confined to the outer half of enamel, it was R1. If radiolucency was observed in both inner and outer halves of enamel layer, including lesions extending up to but not beyond the dentinoenamel junction, it was R2. Finally, if radiolucency was observed as penetrating the enamel and dentinoenamel junction and progressing into the dentin, it was R3. When the progress of caries is on or beyond the R1 stage, it was diagnosed as caries according to the diagnostic criteria based on the prior study.13
The analysis of white spots was performed for QLF-D images taken under the standardized condition using the specialized analysis software (QA2 v1.23, Inspektor Research Systems BV). The analysis patch is set on the three different images obtained from each sample using white spot analysis of the software. The analysis patch was set along the boundary of caries lesion including the sound region, and 5% fluorescence loss automatically calculated. The largest value from these three measurements was determined to be the fluorescence loss (ΔF). According to the QLF-D threshold based on the prior study,18 a tooth was diagnosed as caries when the fluorescence loss was lower than −13.8. The DIAGNOdent threshold was also set on the basis of the prior study,22 and caries was diagnosed when the maximum value was 10 or higher.
To evaluate the intrarater reliability for each detection method, kappa statistics were used for bitewing radiography, and Intraclass Correlation Coefficient (ICC) for QLF-D and DIAGNOdent. Descriptive statistics and frequency analysis were performed to examine the distribution of sound teeth and carious teeth, and the distribution of fluorescence losses in QLF-D and maximum values in DIAGNOdent according to the criteria of caries diagnosis. The Spearman correlation analysis was performed to examine the correlations among bitewing radiography, QLF-D and DIAGNOdent. Also, kappa statistics were calculated to examine concordance of diagnosis among bitewing radiography, QLF-D and DIAGNOdent. Sensitivity and specificity of QLF-D and DIAGNOdent were estimated on the basis of the bitewing radiography diagnosis criteria, and the Receiver Operating Characteristics (ROC) curve analysis was performed to estimate the areas under curves (AUC) for the comparison of the usefulness between QLF-D and DIAGNOdent. Statistical analysis was performed using PASW (PASW statistics, ver. 18.0, SPSS, Chicago, IL, USA) and MedCalc (MedCalc Software, Ostend, Belgium), and the significance level set at 0.05.
RESULTS
The reliability (Kappa statistics) of bitewing radiography was 0.918. The ICC values of QLF-D and DIAGNOdent were 0.843 (95% Confidence Interval: 0.768–0.894) and 0.994 (0.991–0.996), respectively. The analysis of the intrarater reliability for each detection method showed satisfactory level of reliability for all the three detection methods (P < .05).
For a total of 102 teeth, the distribution of sound and carious teeth were estimated. In bitewing radiography with the threshold of R1 stage, the number of sound teeth was 38 and that of carious teeth 64. In QLF-D with the threshold of the fluorescence loss (ΔF) of −13.8, the number of sound teeth was 20 and that of carious teeth 82. Finally, in DIAGNOdent with the threshold of the maximum value of 10, the number of sound teeth was 62 and that of carious teeth 40. Descriptive statistics of fluorescence losses in QLF-D and maximum values in DIAGNOdent showed that the former ranged from −8.55 to −44.5 while the latter ranged from 4 to 99. The mean value of each parameter was −19.47 for the fluorescence loss in QLF-D and 15.14 for the maximum value in DIAGNOdent. The correlation analysis among the three detection methods showed that the correlation coefficient between bitewing radiography and QLF-D was −0.644 and that between the former and DIAGNOdent was 0.448, indicating that bitewing radiography and QLF-D had a higher correlation. The correlation coefficient between QLF-D and DIAGNOdent is −0.382, which indicates that these two also have a statistically significant correlation (P < .05). The assessment of concordance among bitewing radiography, QLF-D and DIAGNOdent using the contingency table based upon the threshold of each detection method shows that kappa statistic of bitewing radiography and QLF-D is 0.443 while that of the former and DIAGNOdent is 0.368. This indicates bitewing radiography has a higher concordance with QLF-D than with DIAGNOdent (P < .05) (Table 2).
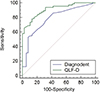
The ROC curve analysis (Fig. 1) in which the bitewing radiography criterion was classification of ‘Sound’ and ‘Caries’ showed that the optimal cut-off value was −17.9 for QLF-D and 11 for DIAGNOdent. At these cut-off values, the sensitivity and specificity were 78.12% and 86.84%, respectively for of QLF-D, and 53.13% and 92.11% for DIAGNOdent. Also, the accuracy of the detection method was very high for QLF-D (AUC = 0.908, 95% CI: 0.835–0.956) and moderate for DIAGNOdent (AUC = 0.784, 95% CI: 0.692–0.859). Therefore, this comparison suggests that QLF-D is more useful, which is statistically significant (P < .05).
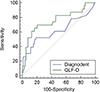
The ROC curve analysis (Fig. 2) in which the bitewing radiography criterion was classification of ‘Sound or Caries into Enamel’ and ‘Caries into Dentin’ showed that the optimal cut-off value was −21 for QLF-D and 15 for DIAGNOdent. At these cut-off values, the sensitivity and specificity were 69.57% and 79.75%, respectively for of QLF-D, and 52.17% and 81.01%, respectively for DIAGNOdent. QLF-D was moderately accurate (AUC = 0.753, 95% CI: 0.659–0.833) and DIAGNOdent was less accurate (AUC = 0.622, 95% CI: 0.521–0.716). This comparison indicates that QLF-D may be more useful, which however is not statistically significant (P < .05).
DISCUSSION
Visual examination and radiography have been used as traditional detection methods for proximal caries. It has been reported that the sensitivity and specificity of visual examination were 0.29 and 0.89, respectively, and increased to 0.36 and 0.98, respectively, when combined with radiography.23 Bitewing radiography is the most commonly used method effective for detecting proximal caries, however, the diagnostic performance of bitewing radiography is affected by the film type, image density and contrast, resolution of radiographic image, geometric characteristics such as magnification and distortion, and the practitioner's imaging technique and ability to read radiographs.24 In contrast, QLF has been a useful diagnostic equipment for detecting early caries and observing the progression and halt of caries lesion.18 Since the lesion in the area where caries is present blocks backscattered fluorescence of dentin, the difference in fluorescence emission between carious lesion and sound areas can be detected and quantified.25 According to a previous study, the correlation coefficient for the lesion depth between QLF measurements and histologic examination, and that between QLF measurements and microradiography were 0.84 and 0.87, respectively.15
In this study, QLF-D images were taken in the directions from buccal, occlusal, and lingual surfaces, and the largest among the fluorescence losses (ΔF) obtained from the three surfaces was used. As a result, more lesions were observed in the buccal, and lingual surfaces than in the occlusal surface, and this was consistent with many previous studies suggesting that it was better to observe proximal caries from the buccal and lingual surfaces than from the occlusal surface.1826 Ko et al.18 suggested that these results were attributed to the difficulties in the measurement of the fluorescence loss due to the thick marginal ridge of the occlusal surface, and occasionally the measurement might be easy in the occlusal surface if the lesion was located close to the marginal ridge. Therefore, when proximal caries is to be detected, QLF-D imaging should be performed at the appropriate location selected depending on the site and extent of caries.
It has been suggested that DIAGNOdent would be useful in detecting caries ranging from early lesions in the occlusal surface to the lesion confined in enamel,27 and this was also confirmed in the results of this study in which the accuracy of DIAGNOdent was higher with the lower diagnostic criteria of bitewing radiography. In a study where DIAGNOdent and bitewing radiography were compared for the detection of proximal caries in deciduous teeth, the reliability of DIAGNOdent has also been reported to be very high and its diagnostic performance was higher than bitewing radiography.14 The results of this study showed that the reliability of DIAGNOdent was the highest among the three detection methods, and this proved a high reproducibility of the DIAGNOdent when detecting caries in the smooth and occlusal surfaces as reported in prior studies.1427
The analysis of the correlation among the three detection methods showed that QLF-D had a higher correlation with the bitewing radiography than did the DIAGNOdent. This result was similar to that in a previous comparative study on the quantification of occlusal caries, in which QLF-D had a higher correlation with the histologic classification or ICDAS than did DIAGNOdent.8 Through these, it could be seen that QLF-D had a higher correlation with other diagnostic methods such as visual examination, radiography and histological examination than did DIAGNO dent in the detection of occlusal and proximal caries. Therefore, it is considered that the use of QLF-D together with visual examination and bitewing radiography is more desirable than DIAGNOdent in order to improve the accuracy of the diagnosis of proximal caries.
When the diagnostic criterion of bitewing radiography was set as classification of ‘Sound’ and ‘Caries’, the sensitivity and specificity of QLF-D in this study were 78.12% and 86.84%, respectively, which were similar to 0.75 and 0.84, respectively, found in a prior study.18 In addition, when the diagnostic criterion of bitewing radiography was set as classification of ‘Sound or Caries into Enamel’ and ‘Caries into Dentin’, the sensitivity and specificity of QLF-D were 69.57% and 79.75%, respectively, which were also similar to 0.64 and 0.88, respectively, shown in the previous studies.18 The results of this study are slightly higher than those of the previous study, and it is considered that these better sensitivity and specificity in this study could be attributed to the diagnosis based on the interpretations of bitewing radiography while histological examination and detection results were compared in the previous studies, leading to slightly lower sensitivity and specificity. In the analysis of the ROC curve to compare the usefulness of QLF-D and DIAGNO dent at the optimal cut-off values where the sensitivity and specificity were balanced, QLF-D was shown to be more useful than DIAGNOdent as the former was found upper left to the latter when the criterion was ‘Sound’ and ‘Caries’. In addition, since QLF-D was upper left to DIAGNOdent at the criterion of ‘Sound or Caries into Enamel’ and ‘Caries into Dentin’, the former could be also considered more useful than the latter at this criterion. However, it was not statistically significant. Through this, it is considered that QLF-D is generally more useful at all stages of caries progression in the detection of proximal caries, and particularly, early caries can be diagnosed more accurately.
Since visual examination is the most affected method by the limitation of such location of the lesion, radiography has been commonly used when detecting proximal caries.18 However, radiography often fails to distinguish between sound tooth surface and carious lesion with a cavity.18 In this in vitro study, it could be seen that QLF-D can detect proximal caries at different stages of the extracted premolars. Ko et al.18 reported that QLF could obtain quantitative data of carious lesion based on the automated analysis, and subsequently would be used as a diagnostic method that could overcome the subjectivity of visual examination and inaccuracy of radiography. Through this and previous studies, it is considered that additional detection using bitewing radiography will be needed for definite diagnosis if caries is detected by the DIAGNOdent. This is because stain, plaque and tartar can cause false positives in the measurement by DIAGNOdent, and this may lead to unnecessary invasive treatments. According to Virajslp et al.,14 since bitewing radiography has a high specificity, a tooth does not need treatment but needs regular check-ups if caries has not been found with bitewing radiography. It is further suggested that the tooth suspicious of caries can be examined by DIAGNOdent with high reliability if bitewing radiography is not available, and if the measured values by DIAGNO dent increase in this case, preventive or operative treatment should be considered.14 In a prior study, it was reported that DIAGNOdent is useful for monitoring the progression and halt of occlusal caries in both deciduous and permanent teeth.28 However, it is considered that more studies are needed in order to monitor proximal caries only with DIAGNOdent.
In this study, the clinical compatibility of commercial light or laser fluorescence tests with the conventional radiography was investigated, and the histologic examination was not performed. Assuming the clinical procedures in daily practice, only the statistical relationships between the diagnostic readings of three different methods were evaluated, using bitewing radiography as a reference test, which was the limitation of this study. To assess diagnostic performances of three detection methods for proximal caries, further studies including standardized histological evaluations are necessary. In addition, studies involving more examiners in consideration of learning curve are needed. Since this study was conducted in vitro and thus has a limitation in applying the results directly into the clinical situation, more in vivo as well as in vitro studies need to be carried out.
CONCLUSION
Within the limitations of this study, the bitewing radiography, QLF-D and DIAGNOdent had excellent reliability. DIAGNOdent showed the highest intrarater reliability among all the detection methods. While all of bitewing radiography, QLF-D and DIAGNOdent showed statistically significant correlations with one another, bitewing radiography and QLF-D had a particularly higher correlation. The concordance of diagnosis of bitewing radiography was higher with QLF-D than with DIAGNOdent.


 XML Download
XML Download