

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Terminal dentition requiring total extraction and complete prosthetic rehabilitation is routinely encountered in prosthodontic practice. An immediate complete denture is a wellestablished clinical procedure whereby a prefabricated prosthesis is directly inserted following teeth removal.1 This approach is applied to maintain the patient appearance and to provide a surgical splint covering the extraction sockets to assist with wound healing and to protect the extraction site. It also helps maintain the vertical dimension of occlusion and lower facial height and provides adequate lip and cheek support through maintaining proper muscle tone and tongue position.2 Immediate complete dentures are preferred by patients as they assist coping with the psychological trauma and social stigma associated with edentulism. However, despite their success and widespread use, immediate complete dentures are associated with several disadvantages related to reduced denture retention, stability, and frequent maintenance. In addition, a fundamental issue with immediate complete denture is the unpredictability of esthetic outcomes due to the inability to have anterior clinical evaluation (teeth try-in) phase.3 Therefore, the teeth of immediate dentures are usually modified or replaced in later stages of the prosthetic treatment when definitive dentures are manufactured, which increases overall treatment time and cost. Developments in CAD/CAM techniques made it possible to digitally design and manufacture complete dentures using milling techniques.4 Recent studies have demonstrated that digitally fabricated dentures are clinically acceptable and comparable in their outcomes to conventional dentures.56 Concurrently, advancements in stereophotogrammetric 3D facial scanning technology have led to the development of compact in office devices capable of capturing the patient's head in full 3D in less than a fraction of a second.7 These systems have been successfully employed to create a virtual patient replica for comprehensive diagnostics and treatment planning in orthodontics and orthognathic surgery.89 More recently, the concept of applying 3D facial scanning for esthetic analysis during the design phase has been introduced in prosthodontics.710 The main idea is to integrate a virtual teeth setup with a 3D replica of the patient face and to digitally evaluate the impact of changing teeth positions, forms, and colors on facial appearance. The 3D design information obtained from this virtual clinical evaluation phase can then be used to fabricate mockups or provisional prosthesis. In the case of immediate denture, a conventional anterior evaluation phase is impossible since the teeth are still present. A virtual setup phase might be a good option to provide the patient and the treatment provider with an idea regarding the facial appearance of the prospective immediate denture. The purpose of this clinical study is to propose a novel digital approach integrating 3D facial scanning in a CAD/CAM workflow to design and manufacture immediate complete dentures.
MATERIALS AND METHODS
Ten patients with terminal dentition in need of total extraction and immediate complete denture were recruited for this study. The participants signed an informed consent and the protocol was reviewed by the institutional review board and the study was conducted with accordance to the declaration of Helsinki. All patients had terminal dentition in both upper and lower jaws and they were in need of an immediate complete denture with no medical contraindication for total extraction surgery. The preoperative planning phase started with obtaining digital photographs from each patient (Fig. 1A). An impression was obtained using Rim-Lock metal trays with extended flanges (DENTSPLY International, York, PA, USA) using irreversible hydrocolloid Alginate and the impressions were then poured into Type IV dental stone to obtain master models (Cavex, Haarlem, The Netherlands). Bite record was obtained using the Avadent silicon bite registration material (Global Dental Sciences, Scotsdale, AZ, USA). The cast models were submitted to a 3D scanning procedure using a laboratory scanner (iSeries DWOS; Dental Wings) to obtain articulated digital cast models (Fig. 1B). The laboratory optical scanner captured point cloud data of the cast model using two camera system and a five axis movement platform. The scanned models were subsequently saved as Stereolithography STL file.
Using the Avadent design software, a virtual teeth setup proposal for a complete immediate denture in a corresponding coordinate system was created (Fig. 1C). The shape of the teeth in the virtual setup was selected from a 3D library available in the design software to be similar to the existing anterior teeth. The software also permits the selection of different occlusal schemes including anatomical, lingualized or flat-on-flat with wide freedom of centric. In this study, a lingualized occlusal concept was selected for all patients.
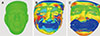
The next step was to acquire 3D facial scanning information to create a virtual patient replica for the 3D clinical evaluation (teeth try-in) phase. Using the in-office 3D facial scanner Pritimirror (Pritidenta GmbH, Leinfelden-Echterdingen, Germany), three different facial scans were obtained from each patient. The first scan was in natural rest position of the head with Frankfurt horizontal plane parallel to the floor (Fig. 2A). The second scan was obtained in a maximum smile position to establish the level of lip exposure (Fig. 2B). The third scan was captured using cheek retractors to expose the labial surfaces of upper and lower front teeth (Fig. 2C). Additional facial scans of the smile line at different exposure levels were also acquired. Subsequently, the three facial scans were aligned to each other using the forehead region as a fixed anatomical reference (Fig. 3). This was necessary in order to bring all facial scans in a single corresponding coordinate system.
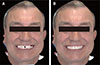
The articulated digital upper and lower cast models were then aligned to the cheek retractors facial scan using four fiducial markers on the labial surfaces of the upper and lower front teeth and the bite registration material (Fig. 4). A surface matching algorithm (iterative closest point) was then applied to bring the 3D surfaces in maximum alignment (Fig. 5). The reference cast models and the virtual wax pattern were then placed in the correct coordinate system with reference to the smiling facial scan using the Pritidenta software (v2.1, Pritidenta, Pritidenta GmbH, Leinfelden-Echterdingen, Germany), which permitted a virtual clinical evaluation phase to be performed (Fig. 6). Following adjustments, a definitive immediate denture proposal was then created using Avadent software and saved for further processing. The denture flanges extended to cover full sulcus depth based on the scan information from the impression to attain adequate retention and stability at the denture bearing mucosa. The digital dentures were submitted to a milling procedure using a 5-axis milling unit (M7 CNC; Darton AG General). First a custom gingiva color puck was milled and then a liquid tooth colored resin was pressed on top of the gingiva puck, which has the cervical outlines already in place. The teeth were then milled after the resin has set. The completed polished dentures were then sterilized and packaged ready for surgical placement (Fig. 7). The remaining dentition was then extracted following administration of local anesthesia and the immediate dentures were fitted intraorally and checked for retention, stability, and occlusion (Fig. 8). The patients were instructed to wear the dentures 24 hours for the first day post-operatively and denture hygiene instructions were provided.
Following three months of uninterrupted healing, the patients were recalled to start the definitive denture treatment. Prior to the clinical consultation, a duplicate upper denture was 3D printed using the digital stereolithography STL information from the immediate denture. In the lower jaw, the posterior teeth were digitally removed from the STL file of the immediate denture to create a bilateral partially edentulous situation. The modified duplicate was then 3D printed using the Formlab 2 printer (Formlabs GmbH, Berlin, Germany), and bilateral wax rims for bite registrations were manually placed. A definitive mucostatic impression was obtained using the Avadent silicone light and medium body impression materials (Global Dental Sciences, Scottsdale, AZ, USA). The bite registration was obtained using guided closed technique with light tapping on the lower chin and the definitive bite was fixated using Avadent registration material (Fig. 9). The patients were submitted to a facial scanning procedure as described above and a new virtual teeth setup was designed. Following approval of the final design, the definitive denture was milled and polished as described above and fitted intraorally (Fig. 10).
RESULTS
Ten patients in need of total extraction and immediate provisionalization with a complete denture were treated in this study using a novel digital approach incorporating facial scanning information in a CAD/CAM workflow. All dentures exhibited satisfactory retention, stability, and aesthetic outcomes with no notable technical or biological complications. The immediate denture design was used as basis for designing the definite complete denture, which accelerated the designing and fabrication procedures.
DISCUSSION
In dentistry, paradigm shifts in the clinical procedures and technical methods used to rehabilitate edentulous patients are currently underway. The myriads of CAD/CAM technologies currently available to plan, design, fabricate, and guide the placement of a removable or fixed, implant-supported prosthesis have revolutionized the field. The soft tissue profile information obtained through 3D facial scanning is undeniably an ideal supplement to the existing scanning technologies. With the facial scan information fused with those obtained from other intra and extra oral scanners, prosthesis design would truly reflect the aesthetic demands imposed by the external profile of the patient, while still adhering to prosthetic constraints. The interplay between aesthetic and prosthetic planning would certainly improve, which in turn will be beneficial to both the patient and clinician. However, since the technology is still at its infancy stages including its applications for prosthodontics, there is an urgent need for more scientific evidence to explore the possibilities. There are several advantages to employing a digital workflow in immediate denture cases. A virtual teeth setup permits seamless and rapid adjustments of tooth size/position and generalized modifications to the occlusal scheme and compensation curves of the dental arch to be applied. These procedures would require a lot of manual labor, time, and cost in a traditional wax-up. Additionally, the virtual setup is digitally stored and thus can be perpetually reused to fabricate a new prosthesis, thereby reducing treatment time and cost in case the prosthesis needs to be replaced. Integrating virtual teeth setup with the facial scan permits immediate inspection of the prosthesis considering facial aesthetics. Similarly, tooth position and morphology can be altered while visualizing the impact on the patient's facial appearance. This would definitely improve on the current clinical procedure of multiple aesthetic teeth try-ins typically required for full mouth reconstructions thereby reducing chair time and treatment cost. Additionally, using this digital approach would improve clinician and lab communication in such cases. Indeed, a technician, who is usually limited to the wax-up on the articulator and selected photographs of the patient, would immensely benefit from this virtual setup, where changes in the restoration design can immediately be visualized on the patient's face. Case communication would also undoubtedly improve.
There were several drawbacks encountered in the current investigation. First, the alignment of the dental cast models and the facial scans depends on the visibility of the labial surfaces of the teeth and the bite registration materials as a common fixed reference. It has been observed in this study that white registration material is unsuited for this digital workflow due to flash light reflection of the camera lens deteriorating the visibility of the bite record.11 Additionally, alignment of the neutral smile and cheek retractor scans rely on the stability of the forehead as a reference. In patients with deep facial grooves, this region can deform when the patient is smiling thereby hampering an accurate registration procedure. Patient related factors including movement during the scan, salivary flow, and facial hair might also influence the accuracy of the scanning and registration procedure.
The technical concept of integrating facial scanning with digital cast models was first introduced by Rangel et al.,12 who used a healthy subject with intact dentition to demonstrate this digital setup for orthodontic purposes. The accuracy of this technical procedure was assessed by Rosati et al.13 on 11 patients, who concluded that integrating facial scans and digital dental cast models is technically achievable. Joda and Gallucci14 presented a case report discussing the integration of cone beam CT, intraoral digital impression, and extraoral facial scan to rehabilitate a patient with two implants in the esthetic zone. A recent pilot clinical study introduced the concept of integrating facial scanning with digital cast models for rehabilitating edentulous patients with implant supported prosthesis.15
CONCLUSION
Ten patients with terminal dentition were treated using a complete digital approach to fabricate complete dentures using CAD/CAM technology. The proposed technique has the potential to accelerate the rehabilitation procedure starting from immediate denture to final implant-supported prosthesis leading to more predictable functional and aesthetics outcomes.








 XML Download
XML Download