

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
To fabricate successful prostheses, it is important to reproduce the interocclusal relationship accurately and transfer it to the articulator.12 Previous studies evaluated the accuracy of these processes234 and reported that errors must be minimized during the bite registration process to reproduce the accurate interocclusal relationship on the articulator.23 The factors that may cause errors during the bite registration process include anatomical complexities, physiological factors, and material properties. Iatrogenic errors caused by bite registration materials can be controlled by skilled clinicians who have a deep understanding of the procedures, appropriate materials and methods.4
Implant-supported fixed prostheses are becoming increasingly common; therefore, various clinical procedures have been attempted using implant components for transferring the interocclusal relationship to the final cast. Savabi and Nejatidanesh5 reported a bite registration method using impression copings. Wicks et al.6 reported the method using healing abutments, and Monzavi et al.7 reported various methods using healing abutments, planning abutments, and impression copings according to the size of the interocclusal space. Recently, a bite impression-taking method was developed allowing simultaneous impression-taking and bite registration for implant-supported fixed prostheses, and various studies have been actively pursued on the properties and accuracies of bite registration materials.891011 On the other hand, few studies have been conducted on bite registration techniques for implant-supported fixed prostheses. Moreover, the accuracy of bite impression copings for implant prostheses, which were introduced recently, has not been fully reviewed. Therefore, this study evaluated the accuracy of various bite registration methods using a three dimensional digital measurement method for implant-supported fixed prostheses.
MATERIALS AND METHODS
The cast of an adult patient with normal occlusion was duplicated to prepare polyurethane maxillary and mandibular casts. The mandibular right second premolar, first molar, and second molar of the cast were removed up to approximately 5 mm inferior to the interproximal gingival margin to form a slightly resorbed residual ridge. At the second premolar site, a 4.0 mm × 7.3 mm fixture (ISII Fixture, Neobiotech, Seoul, Korea) was installed, and 5.0 mm × 7.3 mm fixtures were installed in the first and second molar sites. The implant platforms were located on the gingival level. The prepared cast was occluded and mounted on the semi-adjustable articulator (Hanau Modular Articulator System, Whip Mix, Louisville, KY, USA). This cast was established as the reference model (Fig. 1). All impression taking, cast fabrication, and bite registration processes were conducted by one operator according to the manufacturer's instructions to reduce the errors. For the experimental groups, impression copings were connected to the implant fixtures of the reference model. All coronal parts of the healing (5 mm) and temporary abutments were revealed supragingivally because the fixtures were placed equigingivally. The impressions were then taken with individual trays (Trayplast NF, Vertex Dental BV, Zeist, Netherlands) and polyvinyl siloxane impression material (Delikit Heavy Body, Happi Den, Seoul, Korea). For the group using bite impression coping, however, bite impression copings (Pick Cap Impression Kit, Neobiotech, Seoul, Korea) were connected to the implant fixtures of the reference model and impressions were then taken with bite trays (Dentian bite tray, Seilglobal, Busan, Korea) and polyvinyl siloxane impression material (Delikit Heavy Body, HappiDen, Seoul, Korea) (Fig. 2). Type IV gypsum 100 g (Fujirock EP, GC, Scottsdale, Arizona, USA) was mixed with 20 mL water to fabricate the mandibular casts. Impressions of the maxillary casts were prepared using metal trays and irreversible hydrocolloid impression material (Aroma Fine Plus Normal Set, GC, Tokyo, Japan). Type III gypsum 100 g (Hi-Koseton, Maruishi Plaster, Osaka, Japan) was mixed with 30 mL of water for the maxillary casts. These procedures actually simulated the common clinical procedure.
According to bite registration methods, seven experimental groups were fabricated, as listed in Table 1. The HA and HP group used healing abutments to hold the Aluwax record and pattern resin record, respectively; the HB group used healing abutments to hold the Blu-Mousse record. The TA and TP group used temporary abutments to hold the Aluwax record and Pattern Resin record, respectively; the TB group used temporary abutments to hold Blu-Mousse record. In the case of the BC group, bite impression copings (Pick Cap Impression Kit, Neobiotech, Seoul, Korea) were used for the experimental group whose impression taking and bite registration were done at the same time. The most recently developed bite impression coping was composed of a transfer-type impression coping with various heights and a plastic cap inserted into the impression coping to transfer the position of implants after impression taking. When a short coping is used, impression taking and bite registration can be done simultaneously using a bite tray.
For the groups using healing abutments (Fig. 3), 5 mm high-healing abutments (IS Uni healing abutment, Neobiotech, Seoul, Korea) were connected to the implant fixtures of the reference cast. Aluwax (Aluwax, Aluwax Dental Products, Allendale, MI, USA) was softened homogeneously in a pyrostat at 45℃, according to the manufacturer's instructions.2 Blu-Mousse (Blu-Mousse, Parkell, Edgewood, NY, USA) was mixed with a disposable syringe, and the Pattern Resin was mixed at a ratio of 1 g of powder to 0.6 mL of solution to obtain the bite registration.12 For bite registration, a 1 kg pendulum was placed on top of the articulator11 and removed later when the bite registration material had hardened sufficiently. Complete closure of the articulator was confirmed by inserting an 8 µm thick foil (Shimstock-Foil, Coltene/Whaledent, Cuyahoga Falls, OH, USA) between the incisal pin and the incisal table of the articulator.13
For the groups using temporary abutments (Fig. 4), non-hex type temporary abutments (Plastic UCLA abutment, Neobiotech, Seoul, Korea) were connected to the implant fixtures of the reference cast, and the height of abutments was then adjusted to maintain a 2 mm space against the antagonist teeth.14 Three temporary abutments were connected using Pattern Resin (GC Pattern Resin, GC, Tokyo, Japan) to prepare a platform that could support bite registration materials. Index grooves were formed with semicircular sections to position the bite registration material reproducibly. Using the same technique used for the healing abutment method, an interocclusal relationship was obtained using the three types of bite registration materials. All bite registration materials were trimmed to reveal the cusp tip and left at room temperature for 24 hours under a dried condition before the measurement.15 Fig. 5 shows the overall progress of the groups' classification and experimental methods.
In the groups using healing and temporary abutments, the bite registration record was sitting on the occlusal surface of the mandibular implants. The maxillary cast was occluded on the bite registration record and fixed with sticky wax (Kerr Co., Bioggio, Switzerland) and a tongue blade. Fixed maxillomandibular casts were mounted on the non-adjustable articulators.
In the group using bite impression, impressions were taken using bite trays, and gypsum was then poured until the maxillary and mandibular casts met each other at the most posterior area. After hardening, the casts were removed from the impressions, occluded, and ensured that the posterior gypsum contact was exactly the same before removing the casts from the impressions. The casts were then fixed with sticky wax (Kerr Co., Bioggio, Switzerland) and a tongue blade and mounted on the non-adjustable articulators.
For displacement measurements using a model scanner, scan bodies (Scan body, Neobiotech, Seoul, Korea) were connected to the fixtures on the mandibular left second premolar, first molar, and second molar of the polyurethane model. Digital impressions of the maxillary and mandibular arch and occlusal scheme were taken using a blue light cast scanner (Identica blue, Medit, Seoul, Korea),16 and stereolithography (STL) files of the articulator mounted casts were obtained using digital software (Exocad, Medit, Seoul, Korea). The STL files were evaluated using 3D modeling software (Rapid Form 2004, Inus technology, Seoul, Korea).
The reference point on the mesiopalatal cusp tip of the maxillary right first molar was picked for the reference data set by approximating the virtual plane, which is parallel to the superior plane of the mandibular right-first-molar scan body. This point was immobilized on the reference scan data set to be used as a fixed reference point. The scan data from each group were superimposed with reference data, by registering with three points from the right and left first molar and central incisor. The best-fit alignment was performed using the maxillary arch as a reference. The cylindrical geometry was reverse engineered from the lower first molar scan body of the experimental group data. The distance between the reference point and upper circle center of scan body's cylinder geometry was calculated using the following equation (Fig. 6).

After the experiments had been conducted, the distances between the reference points were measured in each group, and the absolute differences in the distances between the reference points in the polyurethane model (the reference cast) were calculated to determine the means and standard deviations. IBM SPSS software was used for statistical analyses. Normality was tested using the Shapiro-Wilk normality test. The Levene's test was conducted to determine the equality of the variances. One-way ANOVA and Duncan's test was used at the 5% significance level.
RESULTS
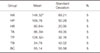
After determining the absolute distance differences between the reference points in the reference model, the distances between the reference points in the experimental group casts were calculated, and compared with the absolute distances in the reference model. Table 2 lists the means and standard deviations of each group. In the TB group, the platform was prepared and Blu-Mousse was used as a bite registration material on top of the platform (34.78 ± 42.02 µm). The BC group, in which bite impression copings for simultaneous impression taking and bite registration (55.14 ± 55.58 µm) were performed, showed least distance differences. In contrast, the HP group, which used the Pattern Resin on top of the healing abutments (169.76 ± 50.28 µm) showed the greatest difference in distance (Table 2).
As a result of statistical analyses of the distance differences, the TB and BC groups showed significantly lower distance differences than the HP group (P = .001).
DISCUSSION
This study compared the accuracies of bite registration for different methods. In previous studies, the accuracy of bite registration materials was measured and compared,911 or the 3D accuracy of casts mounted on an articulator were compared.1718 The latter method was used because it enables the measurements of the groups that do not use the bite registration material.
The 3D accuracy of mounted casts on the articulator can be evaluated in two ways. The indirect method uses the condymeter system for measuring the displacement of a cast,17 whereas the direct method uses reference points on the cast for measurements.18 When the effects of bite registration materials on the accuracy of casts mounted on an articulator were investigated, the direct measurements of cast displacements were found to be more accurate than the indirect measurements of condylar displacements.2 Therefore, the direct method was used in this present study. The mesiopalatal cusp tip of the maxillary right first molar and the center of the superior surface of the scan body on the mandibular right first molar site were used as the reference points, and the distances between these reference points were measured and compared.
The use of an impression material and stone potentially causes dimensional errors. These errors may increase while mounting the casts on the articulator with a physical method.19 Taking an impression for implant fixed prosthesis, the number of the implants, the distance and angulation between the implants, implant-abutment connection type, and preload of the prosthetic component could also influence the accuracy of the impression.20 In this study, all these factors could affect the variation of the distance between the reference points. To minimize the impact of variables other than bite registration methods, impression takings, cast fabrications, and mounting the casts were done made by a single operator according to the manufacturer's instructions.
In the present study, the TB group, in which Blu-Mousse was used on top of the temporary abutment for bite registration, and the BC group, which used simultaneous impressions using a bite tray and bite registration, showed significantly smaller errors than the HP group, in which Pattern Resin was used on top of the healing abutment (P < .05). The reason for the smaller errors in the BC group might be the absence of bite registration material on the cast that triggers repositioning errors. According to Tripodakis et al.,19 when the bite registration material is transferred or repositioned, model mounting errors could be increased as shown in these results. When a full arch impression was taken using an open-mouth impression technique, factors causing error, such as nodule formation on casts, could affect the entire interocclusal relationship compared to the closed mouth impression technique.21 Based on the results of this study, if there are healthy and enough teeth that can induce the maximum intercuspal position, the use of a bite impression coping and bite tray for simultaneous impression taking and bite registration may produce more accurate results.
When casts are mounted on the articulator using a bite registration material, more accurate results can be obtained with a shorter storage period for the bite registration material.18 Acrylic resin bite registration material can be stored for a comparatively long period,22 In contrast, wax exhibits significantly greater linear changes over time due to its high thermal expansion rate.23 Therefore, a wax bite should be applied immediately after bite registration. According to these references, in the present study, experimental casts were mounted on the articulator within 24 hours after bite taking.
Millstein et al.24 reported that more displacement could occur with thicker wax in all directions. In a previous study, an approximately 2 mm space between the platform for bite taking and antagonist tooth was suggested for appropriate results.14 In this study, the groups using temporary abutments and bite taking table produced more accurate results than groups using the healing abutments regardless of the bite registration materials. On the other hand, there were no significant differences between the HA and TA groups, between the HP and TP groups, and between the HB and TB groups under all conditions (P > .05).
A comparison of the bite registration materials showed that the TB groups using Blu-Mousse had significantly smaller errors than the HP groups using Pattern Resin (P = .001), which concurs with previous studies.2526 Because acrylic resin maintains its dimensional stability during storage, it has been used as a bite registration material when a record is required for long term storage.22 Nevertheless, acrylic resin has the limitations of large polymerization shrinkage (Pattern Resin volumetric shrinkage rate: 5.07%) and long hardening time.1227 In this study, Pattern Resin showed the greatest displacement, which was due probably to the large polymerization shrinkage of the acrylic resin. According to Müller et al.,28 more displacements could occur in harder bite registration materials, and the error appears to be larger because of the hardening properties of acrylic resins.
Most recently, additional silicone impression materials have been used widely as elastic bite registration materials because they do not have reaction by-products. Their merits include low resistance to biting, high accuracy, volumetric stability, solidity after hardening,152930 and ease of trimming without deformation.4 Polyvinyl siloxane has excellent reproducibility with respect to micro-tooth structures.31 On the other hand, due to the ‘spring effects’ of polyvinyl siloxane impression material, the vertical dimensions may increase when the cast is mounted on an articulator.3 In the present study, bite registration materials were only positioned on the implant placement sites. To prevent incomplete engagement of the model, bite registration was trimmed away so that only the cusp tips of the antagonist teeth would engage. The relatively accurate results of the groups using Blu-Mousse may have been produced due to the bite registration trimming process, which would prevent the ‘spring effects’ in polyvinyl siloxane material.
A tooth can move physiologically up to 10 – 50 µm horizontally or vertically.3233 The errors measured in this study, in which numerical value itself exceed the physiological range, were the diagonal distance between the reference points that includes vertical and horizontal factors. Therefore, the discrepancies caused by bite registration methods and materials in this study are clinically acceptable because each vertical and horizontal factor separately may be in the physiological range.
The limitations of this study include biological and manipulative errors caused by the temperature differences between the oral cavity and the laboratory, and the errors caused by volumetric changes in the impression and stone materials. Further studies will be needed to consider these factors.
CONCLUSION
Although this study had limitations in in-vitro studies, the groups using temporary abutments to hold Blu-Mousse record and bite impression coping showed greater accuracy than the group using healing abutments to hold the pattern resin record. This study shows the bite registration materials and methods should be selected carefully for implant-supported fixed prostheses.







 XML Download
XML Download