

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Non-vital teeth are significantly different in physical and mechanical properties compared to vital teeth.1234 The fracture resistance of pulpless teeth is influenced by the amount of substance loss,35 the presence of a ferrule,6 the location of the teeth in the arches,7 the type of post and core system,89 the capability of the restorative materials to replace the substance loss,3 and the use of resin cement.1011
Several authors3121314 have emphasized the importance of retaining a maximal amount of sound dentin when restoring endodontically treated teeth (ETT). A post is used when there is insufficient clinical crown remaining. Many studies515161718192021 have demonstrated that the incorporation of a post strengthens a tooth against fracture. Recently, some have rejected the fracture resistance of teeth with posts. A post is essential to retain a core when there is insufficient dentin to support a crown.3222324 Sorensen and Martinoff19 reported no difference in fracture resistance with or without a post. Several in vitro studies2526 have come to similar conclusions. The substantially decreased structural integrity of the tooth during endodontic treatment, preparation of the post space, and placement of the post may increase the failure rate on non-vital teeth.27 The effect of the post is a topic that is extensively studied and yet remains unsettled among various professionals.
There are two types of post in use; custom posts and prefabricated posts. The strength and longevity of a restoration depend on the post system, post length, residual tooth structure, root length, ferrule design, and load.3 The use of prefabricated posts has simplified the restorative procedure because all the steps can be completed chairside with acceptable clinical success.2829 The Parapost® system (Coltène/Whaledent Inc., Cuyahoga Falls, OH, USA) is a parallel-sided, serrated post with a high retention reported as compared to tapered posts.3031
Several studies131416173233343536 have indicated the importance of remaining coronal structure and a circumferential ferrule design with a dentin collar of at least 2 mm in height. To be effective, the ferrule needs to be at least 1 to 2 mm in height to have dentin walls parallel to each other, to completely encircle the tooth, to end on a sound tooth structure, and to avoid invasion of the attachment apparatus on the tooth.37 The importance of the ferrule in restoring ETT has been emphasized frequently in numerous studies.131617363839 The importance of a ferrule has also been observed in a clinical study regarding the survival rate of posts.40 Samran et al.14 reported that to get the advantages of ferrule effect, dentin collar should have a minimum height of 1.5 to 2 mm. In addition, Samran et al.41 noted that the location of the ferrule had no significant influence on final fracture strength.
The purposes of this in vitro study were (1) to evaluate the fracture resistance with various ferrule lengths and (2) to compare the fracture load with and without posts on endodontically treated mandibular premolars restored with prefabricated posts. The first null hypothesis was that there would be no statistically significant difference in fracture resistance according to the ferrule lengths. The second null hypothesis was that there would be no effect of post reinforcement on endodontically treated mandibular premolars.
MATERIALS AND METHODS
One hundred extracted mandibular premolars were selected by the inclusion criteria of free of caries, cracks, or fractures by visual inspections and radiographs, based on a power analysis (G*Power software version 3.1.3; Universitat Kiel, Tranz Faul, Germany). Correct handling of specimens was supervised by Chonnam National University Dental Hospital Institutional Review Board (IRB No.1304/004-001). Hard and/or soft dental debris of teeth were removed using hand scalers, and the teeth were kept in saline during the study except during the operative procedures.
The specimens were randomly divided into 5 groups (n = 20): intact teeth restored with a crown (NR, no root canal treatment); ETT restored with a crown without a post (NP, no post); ETT restored with a prefabricated post, core, and crown incorporating a 0 mm ferrule (F0); ETT restored with a post, core, and crown incorporating a 1 mm ferrule (F1); and ETT restored with a post, core, and crown incorporating a 2 mm ferrule (F2) (Fig. 1, Fig. 2, Table 1).
In each group, the root length (L) from the buccal mid-point of cement-enamel junction (CEJ) to the apex and buccolingual (BL) and mesiodistal (MD) dimensions at the CEJ were measured with a digital caliper (Absolute Digimatic; Mitutoyo Corp, Kanogawa, Japan) (Table 2). The measurements were analyzed with a one-way analysis of variance (ANOVA) to determine significant differences between the groups (P > .05).
Coronal tooth structure was reduced to a height of 6 mm occlusal to the CEJ in NR and NP, at the CEJ in F0, at a height of 1 mm occlusal to the CEJ in F1, and at 2 mm occlusal to the CEJ in F2 (Fig. 2).
Teeth were embedded along the long axis in autopolymerizing acrylic resin (Vertex self-curing; Vertex-Dental B.V., Zeist, Netherlands) at 3 mm apical to the CEJ to simulate an acceptable biologic width between the clinical crown margin and alveolar bone (Fig. 1).
A root canal treatment by the same clinician was applied to groups except for NR. The root canal was prepared within 1 to 2 mm of the apex on a radiograph. The root canal was instrumented with hand files and the step-back technique enlarging the canal to the average #35 K-file (DENTSPLY Maillefer, Ballaigues, Switzerland), irrigated with saline, and dried using paper points (Suredent, Sungnam, Korea). Each canal was obturated with gutta percha points (Suredent, Sungnam, Korea) and a canal sealer (AH plus; DENTSPLY DeTrey GmbH, Konstanz, Germany) by lateral condensation.
Table 3 shows the descriptions for the post and core system used in this study. NR had no post and core. NP was built up with a core at the access opening. The experimental groups (F0, F1, and F2) used prefabricated posts and cores.
One week after the root canal treatment, the experimental groups was prepared with a # 2 Pesso reamer (MANI, Takanezawa, Japan) to remove 9 mm of gutta percha apical to the CEJ. Post space was prepared using a Parapost® drill (1 mm diameter) with a low speed handpiece. A new drill was used for each group during the procedure. The canals were irrigated with water and then dried with paper points and blown air. Paracore® (Coltène/Whaledent Inc., Cuyahoga Falls, OH, USA) build-up was performed according to the manufacturer's instructions, and NRC (non-rinsed conditioner) (Coltène/Whaledent Inc., Cuyahoga Falls, OH, USA) was applied to the canal for 30 seconds. After the material was removed with a dry paper point, air blowing proceeded for 2 seconds, and a mixture of bonding A and B (Coltène/Whaledent Inc., Cuyahoga Falls, OH, USA) (ratio 1:1) was applied for 30 seconds. The excess was removed with a dry paper point, and air blowing proceeded for 2 seconds. A dual polymerizing adhesive resin was applied in the canal with a syringe, and the post was inserted in the canal. After building up the coronal portion, it was set to self-cure for 4 minutes.
All teeth were prepared for a metal ceramic crown with diamond rotary cutting instruments using a high speed handpiece. The same prosthodontist performed all the procedures. The buccal shoulder margin (depth of 1.5 mm) and lingual chamfer margin (depth of 0.5 mm) were prepared with a 6 mm axial wall height. The finish line for the crown was placed at the level of the CEJ. The teeth of the experimental groups were prepared with ferrule lengths of 0 mm, 1 mm and 2 mm, respectively.
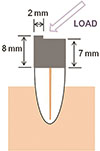
Custom trays were fabricated with light curing resin (Eazipan LC™; Vericom Co., Chuncheon, Korea). Impressions of prepared specimens were made with polyvinylsiloxane (Honigum® light; DMG, Hamburg, Germany) and poured with Type V stone (Suprastone; Kerr, Orange, CA, USA). As shown in Fig. 3, the wax-up for a working model was completed 8 mm above the buccal CEJ and 7 mm above the lingual CEJ for the metal crown. To reproduce the buccal cusp, a protuberance of 2 mm was created on the buccal marginal ridge. Loading was designed to be put on this notch. Wax patterns were sprued, invested, and casted with base metal alloy (Bellabond Plus; BEGO, Bremen, Germany) following the manufacturer's guidelines. The cast crowns were adjusted for passive fit with a silicone disclosing material (Fit Checker®; GC Dental Industrial Corp., Toyko, Japan), and corrected crowns were luted to the teeth with resin modified glass ionomer cement (RelyX luting cement; 3M ESPE, St. Paul, MN, USA) mixed according to the manufacturer's instructions. Each crown was placed for 5 minutes under finger pressure. After the setting was complete, the excess cement was removed with a dental explorer.
The teeth were submitted to 1000 cycles between 5℃ and 55℃ using a thermal cycling machine (The 1100; SD mechatronik GmbH, Miesbacher, Germany) to simulate the degradation of restorations in the oral cavity during cyclic loading, with a dwell time of 10 seconds, as in previous studies.4243
After the thermal cycling test, the teeth were loaded in a universal testing machine (Unitech RB301; R&B Inc., Daejeon, Korea) and placed at an angle of 135 degrees to the axis of the tooth. The load was applied on the protuberance of the buccal cusp with a crosshead speed of 2.54 mm/min (Fig. 3). The fracture load (in N) was measured as the first major load drop occurred.
The data were analyzed with a one-way ANOVA in order to determine the difference of fracture load among groups. Tukey HSD test was used for post hoc analysis. A statistical program (IBM SPSS Statistics 21; IBM, Armonk, NY, USA) was used. A significance level of alpha equal to 0.05 was used for all statistical testing.
RESULTS
The fracture loads in each group are presented in Table 4. NR demonstrated the highest fracture load (262.6 ± 100.8 N). The second highest fracture load was found for F2 (237.7 ± 83.4N). There were significant differences in fracture loads among groups (P < .001) (Table 5).
Fig. 4 shows the post hoc analysis with the Tukey HSD test for fracture load. F2 had a significantly higher fracture load than those of other groups; F0 (41.5 %), F1 (64.2 %) and NP (65.5%) (P < .001, P = .008, P = .011, respectively). No significant difference was detected between the groups NR and F2 (P > .05).
DISCUSSION
Mandibular premolar teeth were selected because they are easy to collect (being extracted for orthodontic reasons) and have a single root. In addition, these teeth are highly susceptible to fracture that may require placement of a prosthesis.7 However, testing other teeth in the dental arch, such as molars or anterior teeth, might have led to different results.
The results of this study support the rejection of the first null hypothesis that mandibular premolars restored with a prefabricated post and resin core had no difference in fracture resistance according to the ferrule length. Increased ferrule length significantly increased fracture resistance for teeth incorporating prefabricated post and core restorations. The 2 mm ferrule group (F2) showed a significantly greater fracture resistance than the 0 mm ferrule (F0) and 1 mm ferrule (F1) groups, and its load was not significantly different from that of intact teeth. Fracture resistance was the highest in the test specimens with the longest ferrules, which is in agreement with other studies.1338 In contrast, some others have observed no effect with a ferrule.44
The second null hypothesis was also rejected. This study indicated that reinforcement of the post had a significant influence on the fracture resistance of the restored teeth, which is in agreement with the other clinical reports.515 However, in this study, it was observed that the 2 mm ferrule group with post (F2) showed a statistically higher fracture resistance than non-vital mandibular premolars without the post (NP), although more coronal tooth structure remained in NP. There were no significant differences in fracture loads between the crowned teeth without the post group (NP) and the group of 0 or 1 mm ferrule with the post (F0 or F1). These results are thought to be due to anatomical characteristics of mandibular premolars, such as the minimal remaining coronal structure after access opening. As a result, incorporation of a 2 mm ferrule with post could reinforce the endodontically treated mandibular premolars.
ETT should not be used as abutments for partial removable dental prosthesis (PRDP).45 Non-vital teeth used as abutments of PRDP have a failure rate 4 times higher than that of teeth not used as abutments.46 Pulpless abutments of fixed dental prosthesis (FDP) have greater stresses in function than single crown abutments.47 Our results showed that there is no significant difference of fracture loading between intact teeth with crowns (NR) and ETT with a 2 mm ferrule incorporating the post and crown (F2). If an endodontically treated mandibular premolar with severe dentin loss is used as an abutment for a PRDP, the post should be recommended for such reinforcement according to results of this study.
Some limitations of this study included the application of finger pressure while maintaining the posts in position, which does not provide a standardized loading force. Although thermal cycling and subsequent static loading were used to measure fracture resistance, the absence of fatigue loading in combination with thermal cycling was another limitation of the study. Clinical observations proved that most fractures in definitive prosthesis occurred several years after restorative procedures. Such failures are generally unrelated to episodes of acute overload but result from fatigue failure. Further research ought to incorporate thermal cycling of the specimens with fatigue loading.
CONCLUSION
Endodontically treated mandibular premolars restored with prefabricated posts and metal crowns with 2 mm ferrule have a fracture resistance similar with that of intact teeth with metal crowns. Moreover, ETT without posts have no significant difference fracture resistance in comparison to those teeth with 0 mm or 1 mm ferrules. Within the limitations of this study, it could be concluded that fracture resistance of endodontically treated premolars was dependent on the length of ferrule, displaying significantly increased fracture resistance in the group with 2 mm ferrule in comparison to the groups with shorter ferrule lengths (F0, F1) and without post (NP).







 XML Download
XML Download