

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The objectives of restorative dentistry include reproduction of the shape and function of the clinical crown, aesthetic reconstruction, and preservation and enhancement of the periodontal tissue and the temporomandibular joint. Knowledge of tooth and gingival morphology lays the foundation for prosthetic treatment, and restorations should be biologically and aesthetically harmonized and balanced around soft tissue.
The factors that affect the aesthetics of smile are the shape, size, color, alignment, and symmetry of teeth, and gingival contour, regularity, and papillary shape of soft tissue. 123 The maxillary anterior teeth, especially, play a dominant role in facial aesthetics because they create facial form by supporting the upper lip. In addition, they cut and tear food, are vital for clear pronunciation, and guide the mandible during eccentric movement. Thus, understanding the shape and contour of the anterior teeth and gingiva is important in order to obtain aesthetic and functional results that are harmonious with the surrounding tissue.4
The morphological characteristics of the teeth and the periodontium are known to be associated with each other. Typically, gingival form is divided into two biotypes, namely thick-flat and thin-scalloped. If the gingiva is thin and scalloped, the tooth has a weak cervical contour and small contact surface, and the contact portions with the adjacent teeth tend to be located near the incisal edge and the interproximal papilla are positioned higher. Conversely, teeth with flat, thick gingiva have a prominent cervical contour and broad contact surface. The interproximal contact is located near the gingiva, resulting in a long contact point short interproximal papilla.12
Various studies have reported the clinical characteristics of gingiva and tooth shape. Olsson and Lindhe reported that gingival recession is more prominent in cases of long and narrow central incisors as compared with wide and short ones.5 The size and shape of teeth differ according to race, region, gender, and dietary habits.6 Average shape of the teeth and gingiva according to race is very useful for prosthodontic restorations. Many studies have reported that these characteristics are different according to race, with differences apparent even among individuals of the same race.678 Most previous studies were done on Anglo-Saxon individuals; few studies24 have examined Korean populations. The existing studies24 about Koreans did not include enough specimens or investigatory sites. The purpose of this investigation, therefore, was to analyze clinical crown dimensions and classify crown shape and gingival type in order to collect anatomical data on the anterior teeth of Korean young adults.
Go to : 
MATERIALS AND METHODS
This study included fifty Korean participants who did not have a history of orthodontic treatment or any special deformities of the jaw and teeth, severe attrition, exodontia, malposition of teeth, periodontitis, or absence of teeth except for the third molar. The study protocol “IRB 2016-08-025” was accepted, and informed consent was obtained from all participants. The participants who had caries in the crown or who had undergone restoration, including interproximal surfaces, were also excluded. Participants ranged in age from 24 to 32 years. Casts used for the study were made from irreversible hydrocolloid impression material (Aroma Fine Plus, GC, IL, USA) and dental stone (New Plastone II Yellow, GC, IL, USA), and a single investigator performed all measurements. The traditional vernier calipers method was used with digital vernier calipers (Mitutoyo Co., Kawasaki, Japan) that are precise to 0.01 mm.
The measured values of tooth dimensions were as follows:
Mesiodistal width of the clinical crown (MDW): The widest mesiodistal width between the interproximal contacts on the labial surface of the tooth (Fig. 1).
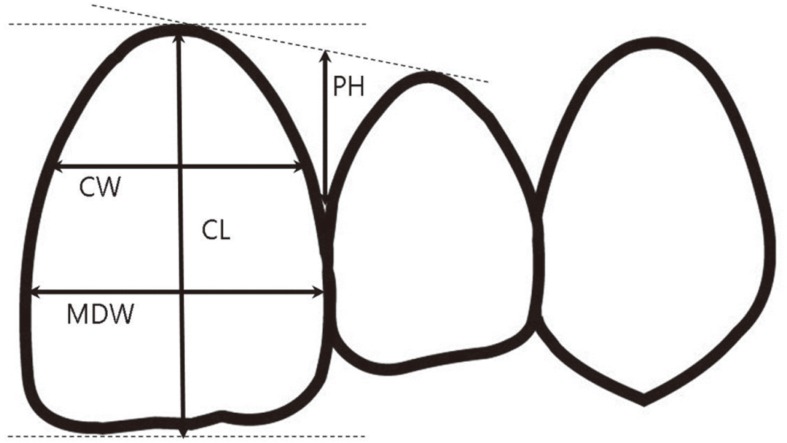
Clinical crown length (CL): The longest apico-coronal distance (parallel to the long axis) of the tooth, from the incisal edge to the gingival zenith.
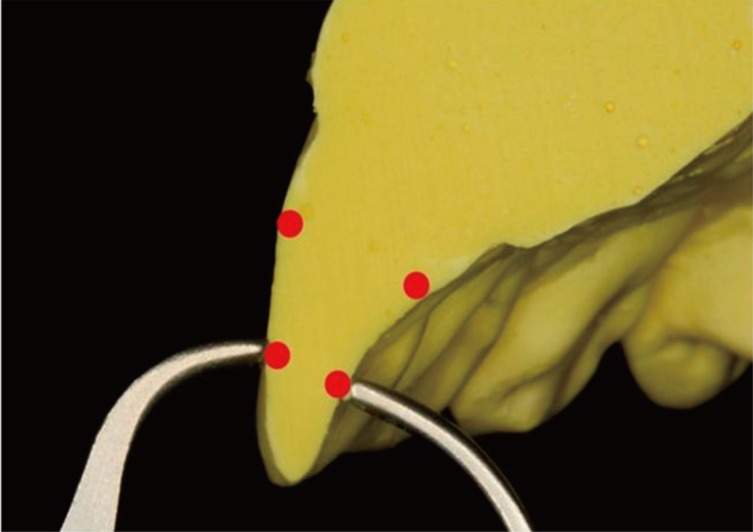
Cervical width of the clinical crown (CW): After evenly dividing the crown length into three parts (incisal 1/3, middle 1/3, and cervical 1/3), the mesio-distal width of the border between the middle 1/3 and cervical 1/3 of the crown length (Fig. 2).
Interdental papilla height (PH): The distance parallel to the long axis of the tooth from the highest point of the interdental papilla to the line that connects the gingival zenith of two adjacent teeth on the distal segment of each tooth.
Crown thickness: After evenly dividing the crown length into three parts, the bucco-palatal thickness of the border between the middle 1/3 and the incisal 1/3 of the crown length (Caliper Iwanson (Hu-Friedy Co., Leimen, Germany) was used in the anterior maxillary incisors) (Fig. 2).
The proportions of parts of the tooth were calculated as follows:
MDW/CL: Mesiodistal width of the clinical crown divided by clinical crown length.
CW/CL: Cervical width of the clinical crown divided by clinical crown length for classification of clinical crown shape.
The tooth shapes are most prominent in the cervical 1/3 of the tooth than in any other part, thus, many previous researchers used CW/CL when studying tooth shape.5910
After calculating the CW/CL ratio, the k-means clustering method, which is an unsupervised learning method for cluster analysis used in data mining to divide data into 3 groups, was used after a validity test to determine the ‘k’ as the group number. Subsequently, one-way ANOVA and Duncan's post-hoc comparison were done to evaluate statistically significant differences between groups. The group that had a small CW/CL value was classified as taper type, while the group with a large CW/CL value was classified as square type, and the group with an intermediate CW/CL value was classified as ovoid type. Gingival shape was classified based on earlier research by Olsson and Lindhe,6 which showed that the morphological characteristics of the periodontal tissues, including the gingiva, impact tooth form. The gingiva associated with taper type teeth were classified as scallop shape and square teeth were classified as flat shape, whereas ovoid teeth were classified as moderate shape. Pearson correlation analysis was performed to examine the relationship between tooth shape and gingival form.
Go to :
RESULTS
The mesiodistal width of the clinical crown (MDW) and the clinical crown length (CL) of the whole dentition are presented in Table 1. The average value of the cervical width of the clinical crown (CW) was 7.17 (± 0.80) mm in the maxillary central incisors, 5.64 (± 0.81) mm in the lateral incisors, and 6.43 (± 0.71) mm in the canines. The average value of the interproximal papillary height was 3.63 (± 0.77) mm in the maxillary central incisors, 3.61 (± 0.88) mm in the lateral incisors, and 3.96 (± 0.97) mm in the canines. For clinical crown thickness, the mean values were 3.14 (± 0.27) mm in the maxillary central incisors, 3.18 (± 0.32) mm in the lateral incisors, and 4.64 (± 0.46) mm in the canines. The CW/CL appeared to be 0.86 (± 0.09) mm in the maxillary central incisors, 0.84 (± 0.13) mm in the lateral incisors, and 0.87 (± 0.10) mm in the canines, while the MDW/CL was 0.73 (± 0.09) mm in the central incisors, 0.67 (± 0.12) mm in the lateral incisors, and 0.71 (± 0.11) mm in the canines. Average values of papillary height are shown in Table 2.


Table 1
Mean values and standard deviations (SD) of crown widths and lengths of the entire dentition
![]()
Table 2
Mean values and standard deviations (SD) for tooth ratio, thickness, and height of interdental papilla of the gingiva in maxillary anterior teeth (in mm)
![]()
Upon dividing the incisors into three groups, we found that the ovoid type made up the largest proportion at 48% of the central incisors and 46% of the lateral incisors. The next largest proportion was the square type, at 29% of central incisors, and taper type, at 36% of lateral incisors. Gingival shape was classified according to tooth shape; thus, the distribution of gingival shape appeared the same as the distribution of tooth shape. The papilla height of each group and other measured values are presented in Table 3. Tooth shape and gingival form were significantly correlated; the correlation coefficient was -0.36 in the maxillary central incisors and -0.37 in lateral incisors (P values < .05).

Table 3
CW/CL ranges, subject numbers, papillary height in the 3 groups divided by tooth shape, and gingival characteristics of central incisors and lateral incisors
![]()
Go to :
DISCUSSION
Prosthodontists should possess knowledge of the standard shape of teeth and gingiva and apply this knowledge to their practice to satisfy patients' desire for aesthetic and functional outcomes. Thus, an understanding of intraoral structures, such as gingiva and mucosa, as well as natural teeth and dentition, is necessary. This study analyzed the shape and size of the clinical crown and gingiva in Korean adults to determine useful standard criteria for prosthodontic treatment.
To study tooth measurements, a plaster model, radiographs, or three-dimensional measurements made with a computer are generally used.8 This study used the plaster model method because the required data were limited to the clinical crown and this method had the advantage of permitting a large number of adult teeth to be observed at the same time.11
This study found smaller length and width values for the maxillary central incisor and canine compared with other research that evaluated patients in North America.12 Many previous studies reported that tooth size was subject to ethnic differences.13141516171819
A study on the maxillary anterior teeth of Koreans20 reported that the average lengths of the central incisor, lateral incisor, and canine were 9.88 mm, 8.43 mm, and 9.65 mm, respectively, with the average width of the central incisor, lateral incisor, and canine being 8.49 mm, 6.88 mm, and 7.76 mm, respectively. These reported values of the length of the central and lateral incisors are similar to the values found in this study.
The labial shape of the maxillary central incisor is usually long and trapezoidal, flared toward the incisal edge and narrow in the cervical portion, and the tooth shape can generally be divided into three groups. A previous study on Korean incisors showed that the triangular form is present in 9.2% of the population, the rectangular form in 11.96%, and the ovoid form in 78.80%.19 These observations were made on extracted teeth in the labial aspect and classified by visual identification. In order to conduct a more objective classification, this study calculated the ratio of the cervical width (CW) and crown length (CL) and divided teeth into three groups. We found that tapered type teeth accounted for 23% of those studied, square type made up 29%, and ovoid type accounted for the remaining 48%. Many studies191021 classified anterior tooth shape using the ratio of cervical width to crown length (CW/CL). Another study22 reported that the width/length ratio of the clinical crown showed little difference based on gender and height, although males had longer and wider anterior teeth than females. It has been suggested that this ratio of values could act as a stable reference.
The labial surface of the maxillary central incisors can be divided into cervical, middle, and incisal parts. Based on inclination, these three parts determine the degree of convexity of the labial surface of the tooth. One of the common mistakes in anterior tooth restoration is over-contouring of the incisal segment in the labial aspect because lingual inclination is deficient after tooth preparation.23 We can estimate these states by the pronunciation of “f” or “v” sounds. If there are problems, the incisal edge will be improperly located over the vermillion border and the restoration will produce an over-contoured incisal edge in the labial aspect. Some researchers have proposed measuring the thickness of restorations between the middle 1/3 and incisal 1/3 to estimate the appropriate incisor thickness, with proposed average values of 2.5 to 3.5 mm.24 This study reported the average thickness of central incisors to be 3.14 (± 0.27) mm, similar to the results of a previous study.24 These results will be useful for the assessment of proper morphology in anterior restorations.
Different biotypes of periodontal tissues tend to react differently during inflammation and perio-surgery. Therefore, considering gingival bio-types is important in order to obtain successful aesthetic and functional results during crown restoration, periodontal treatment, and surgery. The gingival margin of thin-scallop type teeth is recessed because of external stimulation, but thick-flat gingiva tends to form a periodontal pocket. The thin gingiva type tends to occur in cases of gingival recession after nonsurgical periodontal treatment and readily causes problems in the alveolar mucosa.
Regarding the maxillary anterior gingiva, many studies have reported that the morphological characteristics of periodontal tissue and clinical crown shape are related to each other269252627 and that the ratio of cervical width to crown length (CW/CL) in anterior teeth can be used to distinguish between periodontal biotypes.191021 Referring to these studies, we categorized gingival type according to tooth shape and divided teeth according to the CW/CL ratio. The result of correlation analysis between average tooth shape and papillary height signifies that a smaller CW/CL ratio is correlated with a greater papillary height. In other words, tapered teeth are correlated with scallop shaped gingiva, while square teeth are correlated with flat shaped gingiva.
The gingival margin tends to recede toward the apex and passive eruption occurs during the process of aging, so further studies are necessary to determine clinical crown dimensions according to age. The width and thickness of keratinized gingiva in relation to tooth shape is also a necessary avenue of future study.
Go to :
CONCLUSION
This study has established new reference data for tooth size and demonstrated several patterns of tooth shape and different gingival types in Korean young adults. The most frequent gingival form is the ovoid type in maxillary central and lateral incisors. Clinicians should consider these characteristics of the teeth of Koreans during diagnosis and treatment.
Go to :
 XML Download
XML Download