

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Analysis of occlusion is often the first step of prosthetic treatment, especially if extensive reconstruction is needed.1 The likelihood of successful complex prosthodontic procedures is increased when the condylar path of the patient is simulated accurately using an articulator, since this can restore the effective shape of the occlusal surface without the occurrence of occlusal interference.23
The sagittal condylar guidance angle (SCGA) is determined by the condyle and articular disc traversing the contour of the glenoid fossa and the articular eminence. The SCGA can be measured using the anterior bite registration method, radiographically, or using a jaw movement recording device.24 The SCGA on an articulator is determined using either the protrusive or lateral interocclusal records of the patient.456 Christensen's method was introduced in 1905 as a way to obtain the SCGA using wax directly on the articulator.7
Several previous studies have investigated the use of radiographic images for measuring the SCGA.6 However, most studies used panoramic images, with very few using CBCT images.
Tannamala et al.8 found that the SCGA differed by 2 - 4 degrees between using panoramic images and the protrusive occlusal record, but they did not analyze the correlation between these measurements. Panoramic images are often not accurate for measuring the SCGA due to several structures being superimposed. The use of CBCT has recently become much more common, and when measuring the SCGA using CBCT, more reliable results can be expected.
Shreshta et al.4 found that the SCGA differed by 9 - 10 degrees between using CBCT images and the protrusive occlusal record, with Pearson's correlation coefficients of 0.423 and 0.237 on the right and left sides, respectively. They measured the SCGA using 3D CT reconstruction, which might not be accurate due to overlapping structures in the glenoid fossa area.
The use of CT may produce different results depending on which cross-section images are used for the measurements. The SCGA obtained using radiographic images can also vary according to the type of radiation and the cross section used for the same CBCT data. Moreover, the image processing methods used in previous analyses have not been described in detail. Therefore, in this study, we used both panoramic and CBCT images, with the latter subdivided into two types according to the method the images were obtained.
The recent increase in the popularity of CBCT radiography has resulted in prosthodontic implant treatment planning using CBCT images becoming more common. Digital CBCT scans have made them safer, more accurate, and cheaper, resulting in their widespread application in many areas of dentistry.910 This has increased the availability of useful data in radiographic images. Using radiographic images to measure the SCGA has many advantages, especially in cases where there are difficulties measuring this angle using the protrusive occlusal record or a virtual articulator. If a virtual articulator for designing a crown can be included in CAD-CAM, this would make the clinical procedure for occlusal adjustment easier, and make the occlusion more effective. Hence, SCGA measurements obtained from radiographic images may be clinically usefulness.
The present study compared SCGAs as measured in three types of radiographic images (panoramic, CBCT panoramic-section, and CBCT cross-section images) with the values obtained using the protrusive occlusal record.
The null hypothesis was that there were no significant differences in SCGAs between radiographic imaging methods and the protrusive occlusal record.
Go to : 
MATERIALS AND METHODS
The study involved 20 patients aged 20 - 40 years (mean age 32.15 years) with a complete set of teeth, class I molar relation, and 2 - 4 mm of overjet, with available anterior guidance within the normal range and no temporomandibular disorders. This study was conducted after receiving Institutional Review Board approval.
Irreversible hydrocolloid impressions (Andante; Cavex, The Netherlands) were taken and immediately poured in stone (Fuji Rock; GC, Lluven, Belgium). The casts were then mounted on a semi-adjustable articulator (Artex; Amman girrbach, Koblach, Austria) with a face-bow transfer. In the protrusive occlusal record, the patient was made to sit upright on a chair and made a bite registration on the edge-to-edge bite position (Fig. 1).34 In this position, softened 3-mm-thick Aluwax was applied on the protrusive occlusal record resin tray and protrusive occlusal record was prepared. The SCGA was determined using the protrusive occlusal record on an articulator, with two operators calculating the average after making two measurements independently.

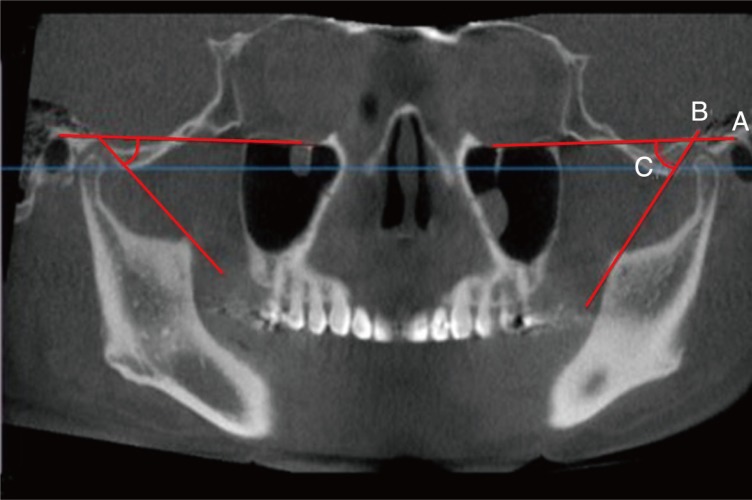
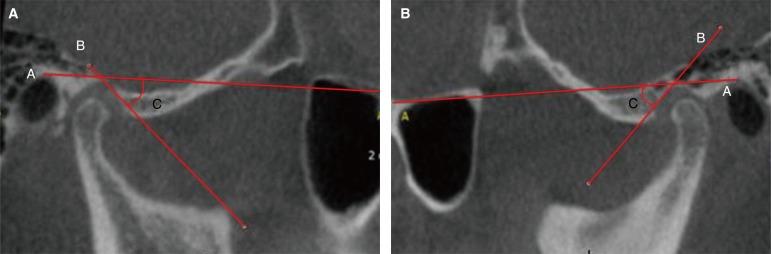
Panoramic (15.1 seconds, 10 mAs, 71 kVp; Kodak CS 9000; Carestream Dental, Sydney, Australia) and CBCT (8.9 seconds, 18.54 mAs, 120 kVp; KaVo 3D eXam; Kavo Dental, Biberach, Germany) images were obtained according to the manufacturers' instructions. CBCT data were used to reconstruct images using the OnDemand3D software (CyberMed, Seoul, Korea), which were converted into the DICOM format. On panoramic and CBCT images, the Frankfort horizontal plane was marked by joining the orbitale and porion. The most-superior and most-inferior points of the curvature were identified to determine the mean curvature line. The angle formed from the intersection of the mean curvature line and the Frankfort horizontal line was measured (Fig. 2, Fig. 3). CBCT images were divided into panoramic-section and cross-section images. Based on the axial section at 4.5 mm below the plane of the superior part of the condyle, the CBCT panoramic section was determined with a sectioning line at the middle part of the both condyle and the nasal tip (Fig. 4, Fig. 5), and the CBCT cross section was determined by sectioning at the center of the condyle cross section (Fig. 6, Fig. 7). The CBCT image was converted into the DICOM format using OnDemand3D software (CyberMed, Seoul, Korea), and SCGA was measured on the CBCT image in the same manner as for the panoramic images. Each measurement was performed twice by two operators. Average value was used.
 | Fig. 2Measuring the SCGA in a radiographic tracing image. Line A: Frankfort line (Or - P), Line B: Most-superior and most-inferior points of the curvature, Or: Orbitale, P: Porion, Con: Condyle, Angle C: Angle made by the intersection of lines A and B.
|
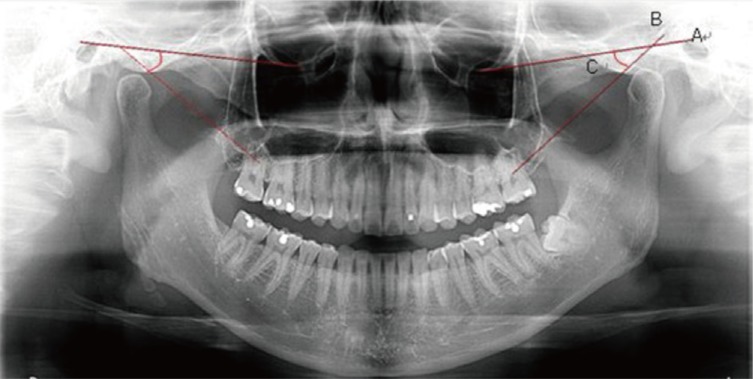 | Fig. 3Measuring the SCGA in panoramic images. Line A: Frankfort line (Or - P), Line B: Most-superior and most-inferior points of the curvature, Angle C: Angle made by the intersection of lines A and B.
|


Go to :
RESULTS
The data were analyzed by the t-test, Pearson's correlation test. The results obtained in statistical t-test comparisons of the methods between the right and left sides are presented in Table 1, while Pearson's correlation test comparisons between the methods are presented in Table 2. The reliability of the measurements was confirmed using Cronbach's α values. The SCGA was significantly higher for the panoramic method than for the protrusive occlusal record (by 8 - 9 degrees), and for the CBCT method than for the protrusive occlusal record (by 5 - 6 degrees). Strong correlations were identified between the measurements using all types of radiographic images and the protrusive occlusal record.


Table 1
Comparisons of right and left SCGAs (in degrees) for the different methods
![]()
Table 2
Comparisons between different methods using Pearson correlation
![]()
Go to :
DISCUSSION
The null hypothesis was rejected since significant differences were found in the SCGA between radiographic imaging methods and the protrusive occlusal record.
As mentioned in the Introduction, these results are similar to those of a previous study, reporting that radiographic measurements were 2 - 10 degrees higher than those from the protrusive occlusal record.48 In this study, the CBCT value was closer to the protrusive occlusal record value than the panoramic value, which may have been due to overlap in the panoramic images.
Christensen and Slabbert reported that SCGAs obtained radiographically are higher than those obtained from intraoral records.1112 However, if the difference between two methods is consistent, a clinically applicable SCGA can be obtained by adjusting the value measured using radiographic images. There were strong correlations between the SCGAs measured radiographically and using the protrusive occlusal record. Cronbach's α was high for all of the methods, indicating a high internal consistency. Therefore, measuring the SCGA using radiographic images might indeed be a useful method.
Previous studies found that intraoral methods of SCGA measurement have lower levels of reproducibility,131415 which is attributable to variations between the instruments and operators.16 The error in protrusive occlusal record measurements can be large due to various factors.1718 Previous studies reported that the thickness of the material used for recording the mandibular movement affects the accuracy.5 The thickness of the wax was therefore kept uniform in the present study, and adjusted according to each subject so as not to be too thick.
For SCGA measurements using CBCT, the CBCT images were divided into two types and each image followed a specific measurement protocol. Each CBCT image was divided into a panoramic section and a cross section. The SCGAs differed with the height of the axial section, and so the axial height needs to be determined for each person to ensure that standardized values are obtained.
Panoramic radiography and CBCT are now widely used in diagnoses. We used CBCT to determine the relationships between protrusive occlusal record and radiographic measurements. If SCGA measurements can be applied to the virtual articulator setting in a CAD-CAM process, this would greatly increase their clinical application.19
The protrusive occlusal record and CBCT imaging method were found to be comparable in this study. The panoramic measurements of the SCGA were 8 - 9 degrees higher than the protrusive occlusal record measurements, with CBCT panoramic-section and CBCT cross-section measurements being 5 - 6 degrees higher. Therefore, in this study, subtracting 6 degrees from the SCGA measured using CBCT images seems to be reasonable for clinical applications. However, further studies with larger samples are needed to confirm the present results.
Go to :
CONCLUSION
Strong correlations were detected between the SCGAs obtained using radiographic images and the protrusive occlusal record. The radiographic measurements were 5 - 9 degrees higher than those made using the protrusive occlusal record : by 8 - 9 degrees for panoramic measurements and by 5 - 6 degrees for CT measurements.
Go to :
 XML Download
XML Download