

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The accuracy of the intraoral impression is a key factor when performing indirect restorations and influences the outcome of reconstructive treatments considerably. Digital impression techniques have been established in the clinical workflow during the past decade, with an assumed prevalence of 5 - 10% in clinical practice of developed countries.1 It was demonstrated that intraoral scanning was preferred by patients2 and resulted in shorter working time than conventional impressions.3 The precision of digital impressions was shown to be comparable to conventional methods,45 but certain limits still exist particularly with long-span restorations due to a distortion from pictures stringed together in arc.6 Further, the reproduction of subgingival finishing lines is still challenging for both methods; it is handled with mechanical retraction by cords removed just before conventional impression materials are injected, while these regions have to be visible during the period of the optical scanning procedure.7 Thus, even though the use of digital impression is continuously increasing, conventional techniques are still most commonly used on a routine basis.8
Addition-cured silicones are the most popular elastomers used in dental practice these days.9 They can be applied with various impression techniques. The twin-mix technique uses two materials of different viscosity. While a low viscosity wash is placed around the teeth, a stock tray is loaded with a putty material, inserted intraorally, and both materials are allowed to set simultaneously. However, concerns have been raised because the uneven bulk of impression material may be subjected to distortion.10111213 Furthermore, the putty may displace the wash in areas where accuracy is essential, and tray removal may be hampered in the event that putty flowed into the interdental spaces.14
To overcome these problems and improve accuracy, custom trays were proposed. The reduced volume of the impression material associated with this technique allows the application of low-viscosity materials. However, the fabrication of a custom tray requires an additional step including a dental laboratory. According to a survey from 1980, only one third of dentists used custom trays routinely.15 More recent data reveals a significant disparity in the utilization rate of custom trays between general dentists (68%) and prosthodontic specialists (100%).16
For the separating foil impression technique, a putty material is used to individualize a stock tray. A preliminary impression is taken with a foil laid over the mixed putty in a stock tray, which is moved intraorally until setting to create a space towards the dentition. After removal of the spacer foil, a second impression is produced using a lower viscosity wash, which reproduces the necessary surface details.14 Different spacer materials have been proposed for this technique including polyethylene and cellophane foils.17
According to in vitro studies, the foil technique led to more uneven dimensional changes compared to other techniques, in which the wash material space was standardized.181920 The inferior accuracy of foil impressions was attributed to a suboptimal adaptation of the foil particularly in the interproximal areas, resulting in considerable variations of the wash space.21
Recently, a new polyolefin foil (Plicafol, GS Folienfertigung, Lebach, Germany) with 0.2 mm thickness and high elasticity has been introduced. Due to its flexibility, the foil is claimed to adapt around the irregular shapes and surfaces of the dentition. Thus, the foil may have ideal properties to create a uniform space for the wash material, but to date no study has investigated the impression accuracy of this approach.
The aim of the present in vitro study was to compare the accuracy of the separating foil impression technique with two established impression methods by investigating the dimensional accuracy of epoxy resin casts.
MATERIALS AND METHODS
A machined mandibular complete-arch metal model with special modifications served as the master cast. This model was designed with both mandibular first molars missing. Both left and right second molars and first premolars and a left second premolar were replaced by stainless steel cylinders with occlusal reference lines (Fig. 1A). On the right second premolar, a modified overlay preparation was grinded with reference lines on the occlusal plane (Fig. 1B).
During the entire experiment, the room temperature was kept constant at 23℃. Three different impression techniques were used as follows (Table 1):
In group MET, a prefabricated non-perforated metal tray with retentive rims (Ergolock 411, Omnident, Rodgau, Germany) was used. The inner surface of the tray was coated with a thin layer of adhesive for silicone-based impression materials (Coltene Adhesive, Coltene-Whaledent, Altstätten, Switzerland) and left to dry for 3 minutes prior to use. A single-step impression technique was applied using a hand mixed high-viscosity material for the tray (Affinis Putty soft, Coltene-Whaledent, Altstätten, Switzerland) in combination with a low-viscosity material in an automix cartridge system (Affinis Regular Body, Coltene-Whaledent, Altstätten, Switzerland) injected onto the onlay preparation and to the occlusal reference grooves. A prolonged setting time of 10 minutes was selected for room temperature conditions (23℃), which corresponds to a 3-fold setting time recommended for intraoral use by the manufacturer.
For group CUS, a custom tray was fabricated with visible light-cured resin material (Individo Lux, VOCO Cuxhaven, Germany) according to the manufacturer's instructions, maintaining a circumferential distance of 2 - 3 mm to the bucco-oral surfaces.22 The inner surface of the tray was coated with Coltene Adhesive (Coltene-Whaledent). Impressions were performed with a single phase approach using low-viscosity material (Affinis Regular Body, Coltene-Whaledent). The same custom tray was cleaned with alcohol (90%) after model casting and subsequently used for all impressions in this group.
For group SEP, the prefabricated metal tray, which was also used in group MET, was applied after cleaning and coating the inner surface with Coltene Adhesive (Coltene-Whaledent). A preliminary impression was performed with putty material (Affinis Putty soft, Coltene-Whaledent) and a separting foil (Plicafol, GS Folienfertigung, Lebach, Germany). After positioning, the tray was moved every 20 seconds in an occlusal direction with slight horizontal movements to avoid the replication of any undercuts and to facilitate easy removal. After a setting time of 5 minutes the tray was released from the model and the separation foil was removed. The second-stage impression was taken with a low-viscosity material (Affinis Regular Body, Coltene-Whaledent), which was thoroughly applied to the relevant structures on the master model and on the already set putty impression. The second impression was allowed to set for 10 minutes.
For impression removal, a standardized approach was applied mounting the metal model with the impression tray in a universal testing machine (Instron 1000; Instron, High Wycombe, UK). The tray was loaded in tension using a 360 mm/min crosshead speed. All impressions were stored at room temperature (i.e. 23℃) for 24 hours before being poured in epoxy resin (Exakto-Form, Bredent, Senden, Germany); epoxy resin was selected due to its high accuracy (linear shrinkage 0.17%) and stability according to the manufacturer's instructions. All casts were numbered to facilitate blinded measurements without knowledge about group affiliations.
Six different distances (four intra-abutment distances and two inter-abutment distances) were defined and measured on all casts and the metal master model as reference (Fig. 2). All measurements were performed by one experienced examiner using a microscope (Leica M7A, Leica, Solms, Germany) in combination with a digital camera and a calibrated measuring software (Leica IM 1000, Leica). On the metal master model, each distance was measured 6 times, and the corresponding means served as reference values. On each of the dental casts, every distance was measured three times and means were calculated for each cast for further analyses.
Data were analyzed with the JMP software package (SAS institute, Cary, NC, USA). The differences of each evaluated distance (in microns) between the metal master cast and the test group were calculated and expressed as mean with one standard deviation (± SD). The 95% confidence intervals of the means were calculated and significant difference between the experimental groups was assumed when confidence intervals did not overlap. In addition, deviations were calculated as percentage of the respective reference values.
RESULTS
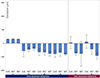
Overall, the smallest dimensional changes compared to the reference values were detected in group CUS, varying between -78.86 µm and 30.84 µm corresponding to -2.32 and 1.53% of the master cast dimension (Table 2). For the intra-abutment distances (d1 - d4), no significant differences were detected among the three experimental groups. For the inter-abutment distances, group CUS showed a significantly higher dimensional accuracy for dimension x1 with -0.02% compared to MET (-0.03%), and for dimension x2 with -0.08% compared to SEP (-0.55; Fig. 3).
DISCUSSION
The current in vitro study investigated the dimensional accuracy of three impression techniques and documented a significantly higher accuracy for inter-abutment distances with custom trays and single-phase impression compared to the wash technique and the 2-stage technique with prefabricated metal trays. However, the intra-abutment distances did not differ significantly among the experimental groups.
For the present investigation, a solid custom made metal master model was preferred over an acrylic model, as used in other studies,2324 to avoid any source of error caused by mobile teeth or dimensional changes due to variations in ambient temperature. To obtain reliable and clinically relevant results, all efforts were made to simulate a realistic intraoral impression procedure. Missing teeth and an intracoronal tooth preparation facilitated measurements of both intra- and inter-abutment distances to assess dimensional accuracy. A standardized approach was chosen to remove the tray from the master model in order to exclude any distortion resulting from variable handling procedures. All measurements were performed with an established high accuracy setting. Most in vitro studies focusing on the accuracy of impressions used simplified master models with 1 to 3 truncated cone-shaped metal forms to simulate abutment teeth with full crown preparations.181920242526272829 Such idealistic and highly standardized settings facilitated a perfectly controlled space for the wash material. Their ability to reproduce the clinical situation were, however, limited due to missing undercuts and interproximal areas, and the documented accuracy was potentially overrated. Thus, it is not surprising that in the present investigation the measured values in all 3 groups showed comparatively greater variations and slightly higher discrepancies.
A shortcoming of the present analysis was that the impressions taken were not immersed in disinfecting solutions. In clinical settings, disinfection of the impressions is mandatory and possibly has an effect on the impressions' precision.30 However, since identical materials and storage conditions were applied in all groups, the potential influence on the current results might be negligible.
The current data revealed that the 1-step putty-wash technique resulted in similar intra-abutment dimensional accuracy as the custom tray and the 2-step foil techniques. A possible detriment of this stock tray impression with simultaneous setting of the putty and the low-viscosity wash material is that the actual thickness of the wash material is difficult to control. Therefore, essential areas of the tooth preparation including cervical margins may be partly recorded in putty-instead of wash material, resulting in reduced marginal accuracy.1731 In contrast, a randomized controlled clinical trial demonstrated that best reproduction of subgingival finishing lines was performed with a custom tray based 1-step putty-wash technique, when compared to a monophase impression or a 2-step impression, in which undercuts were removed and drains were created after the first impression stage to improve the flow of the low viscosity material.32
The use of custom trays is regarded as the gold standard and is adopted by the majority of prosthodontic specialists.16 A custom tray ensures constant material thickness and facilitates a dental and/or mucosal support. A variety of in vitro studies demonstrate that a uniform spacer thickness not exceeding 2 mm offers ideal preconditions for accurate impressions in terms of dimensional accuracy and marginal precision.192023252728 Several in vitro studies showed that a uniform thickness of the impression material was achieved by using copings with precise dimensions on the abutment teeth. However, the fabrication of a custom tray possibly results in considerable variations from uniform thickness.33 In the present investigation, the custom made tray was fabricated in a realistic setting, thus showing the above mentioned limitations concerning a uniform tray space. This may have additionally impaired dimensional accuracy compared to other studies with perfectly controlled material thickness. However, the recorded mean values in this group (< 80 µm) fall into a range which is considered to be clinically acceptable.34
The separating foil technique with Plicafol was used to fabricate a well-fitting putty tray as a simple chairside alternative to custom trays. With this separating foil technique, sufficient space for the regular body material should ideally remain around the oral structures. However, a uniform and consistent wash space cannot be guaranteed. In a recent study, a polyethylene foil was used to create a putty tray and a light-bodied polyvinyl siloxane was used as regular body material.18 Although a highly standardized setting with truncated metal cones was used as master model, the mean deviations varied between 132 µm and 260 µm for the intra-abutment, and between 96 µm and 119 µm for inter-abutment distances.18 In the current study, smaller deviations from the master model were observed ranging from 31 µm to 82 µm for intra-abutment and 77 - 92 µm for interabutment distances. While deviations of intra-abutment distances did not differ significantly among the groups, the highest deviation of all measured distances was detected in group SEP for both inter-abutment distances.




 XML Download
XML Download