

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
PMMA (polymethyl methacrylate), a denture base material, is more aesthetically pleasing and easier to construct and repair compared to metal, as well as forming superior chemical bonds with resin artificial teeth. However, low-mechanical-strength resin bases are vulnerable to deformation during the mastication process and to impact failures.1 Therefore, reinforcing materials improving the mechanical properties of complete dentures are required. Currently, in clinical practice, metal frameworks are primarily used as reinforcements to improve the fracture resistance, volume stability, and precision of complete dentures. el Ghazali et al.2 reported that metal frameworks reduced the functional deformation and problems of the supporting tissue. However, metal frameworks are heavier and require more complicated fabrication processes compared to resin bases. Further, because they are made from alloys, the possibility of hypersensitivity cannot be excluded.3
Glass fiber has been used as a reinforcement material in many fields. Because the material can bend without breaking, studies have focused on the use of glass fiber as a replacement for metal framework in dentures to improve the reparability of failed dentures.45678910 A complete denture with a glass fiber framework has a shorter fabrication time, lighter weight, and better aesthetic features than one using a metal framework, benefiting dental technicians, dentists, and patients. However, thus far, few experimental and clinical studies have investigated the mechanical properties of glass fiber mesh-reinforced complete dentures. In particular, glass fiber mesh-reinforced and metal mesh-reinforced complete dentures have rarely been compared regarding their fatigue resistances and long-term prognoses.
Previous studies on the chewing force of patients with maxillary and mandibular complete dentures have reported varied results because they lacked controls for conditions, such as gender, development of the masseter muscle, and residual ridge, but the average fatigue load has been cited as 43 - 100 N.1112 Some studies have reported that loading may occur in normal chewing processes at a rate of 1,000 cycles per day,13 but Wiskott et al.14 reported mastication rates reaching 1,000,000 cycles per year.
This study evaluated the effects of reinforcing materials on the fracture resistance of complete maxillary dentures by applying dynamic fatigue loading, followed by compressive loading, to maxillary resin dentures reinforced by glass fiber mesh or cast Cr–Co alloy metal mesh frameworks.
MATERIALS AND METHODS
Three types of maxillary complete dentures were constructed: unreinforced acrylic resin-based (control group; R), Cr–Co metal mesh-reinforced (M), and glass fiber mesh-reinforced (F) (Table 1). A total of 45 master casts were constructed using a silicone mold of fully edentulous maxilla (H3-402-U, Nissin Dental products Inc., Kyoto, Japan), duplication silicone (Elite double 22, Zhermack SpA, Badia Polesine, Italy), and high-strength plaster stone (GC FUJIROCK EP, GC Europe N.V., Leuven, Belgium) (Fig. 1A). The frameworks were designed to cover the palate and extend 2 mm from the alveolar crest toward the vestibule and 6 mm ahead of the posterior border of the cast. A 0.5-mm-thick sheet wax (Stippled Wax, Daedong Industry, Daegu, Korea) was used for relief, and 5-mm-wide tissue stops were formed at the positions of the canine and the first molar (Fig. 1B). Then, the silicone mold with relief was constructed using duplication silicone to duplicate the wax relief in the cast.
Fifteen refractory casts were fabricated using an investment material (Dentivest partial, Sinji, Seoul, Korea) and the silicone mold with relief. After being placed in molten dipping wax (Ticonium Bees Wax, CMP Industries LLC, Albany, NY, USA) for 10 seconds, the refractory cast was placed in a 150℃ furnace for 60 minutes and then cooled at room temperature. A wax pattern of the metal mesh was created by the same technician on each cast using mesh-pattern wax (Dental wax saddle, Dae-dong Industry) and then flasked. The metal mesh frameworks were castusing a Cr–Co alloy (Ticonium 1000, CMP Industries LLC) and polished (Fig. 2A).
Fifteen working casts were fabricated with dental stone (Mega Gemma 23, Samwoo Co. Ltd., Seoul, Korea) and the silicone mold with relief. The glass fiber mesh product (SES Mesh, INNO Dental Co., Seoul, Korea) used for this study was manufactured from silane-treated twisting E-glass preimpregnated in a light-curing resin at a thickness of 0.45 mm (manufacturer's data). Fifteen glass fiber mesh frameworks were fabricated following the manufacturer's instructions. After the fiber mesh was positioned on the working cast with an applied resin separating agent (Acrosep, GC Corp., Tokyo, Japan), both were placed in a vinyl bag with suction using a vacuum device (SES 5100-G, INNO Dental Co.). The fiber mesh was polymerized for 4 minutes with a light-polymerization unit (SES curing unit, INNO Dental Co.). After the cast and the fiber mesh were removed from the vinyl bag, a self-curing acrylic resin (Vertex Self Curing, Vertex-Dental B.V., Zeist, Netherlands) was injected into the stop spaces. The fiber mesh, separated from the cast, was trimmed with scissors to match the form of the metal mesh (Fig. 2B). Each of the metal and fiber mesh frameworks was weighed on a digital scale.
The maxillary resin complete denture, used as the control, was constructed in the usual manner on the master cast using heat-curing denture-base acrylic resin (Vertex RS, Vertex-Dental B.V.) and cusped resin artificial teeth (264-66, 32M-66; Biotone, Dentsply, Petropolis-RJ, Brazil). The thickness of the denture base was 2 mm. After the denture was polished, a silicone mold was constructed for wax denture duplication, from which 45 wax dentures were replicated. The resin complete denture, metal mesh-reinforced complete denture, and fiber mesh-reinforced complete denture were constructed in the usual manner, 15 for each type. When the denture base resin was applied, the frameworks could be deformed or moved. To prevent this, the dental technologist used quick-drying glue on the stops of the frameworks and packed the resin carefully. After the dentures were weighed, the occlusal surfaces of the posterior teeth were adjusted to stabilize the denture on the floor with a level instrument. The dentures were then stored in water at 37℃ for 6 months.
Fatigue testing was performed using a chewing simulator (CS-4.8, SD Mechatronik, Feldkirchen-Westerham, Germany). Loading at 80 N was applied by a stainless steel T-bar-shaped jig to the second premolar on each side at 1.6 Hz for 300,000 cycles in 37℃ water. The maxillary edentulous cast was made with polyurethane epoxy resin material (Polyurock, Cendres Metaux SA, Bern, Switzerland). The central region of the palate between the two second premolars was protruded by 1 mm in a dome shape with a diameter of 1 cm (space maker). This prevented contact between the residual ridge of the cast and denture base for the functional deformation of the denture (Fig. 3). After fatigue testing, the presence or absence of cracks and failures was recorded for each complete denture.
A universal testing machine (RB-306, R&B Co. Ltd., Daejeon, Korea) was used to compare the fracture resistances of the complete dentures made with different reinforcing materials. After each complete denture was positioned with the occlusal surface oriented downward, loading was applied at a crosshead speed of 5 mm/min using a stainless steel ball of 1.5 cm in diameter. The load was applied on the tissue surface at the point where the palatal midline of the complete denture crossed the line connecting the second premolars on each side, and the fracture resistance was recorded.
The failure modes were categorized as complete fracture into two or more parts, incomplete fracture with framework fracture, and framework deformation only. Other special features were also analyzed.
One complete denture exhibiting a fracture surface in the resin base or the reinforcing material was randomly selected from each group, and specimens were constructed from these selections to perform fractography. The fractured surface of each specimen was coated with platinum (30 mA, 60 s; Leica EM SCD005, Leica Mikrosysteme GmbH, Wien, Austria) and observed under a scanning electron microscope (SEM; Inspect F50, FEI Co., Hillsboro, OR, USA) at various magnification ratios from low to high (20 kV; 100×, 400×, and 1,000×).
For statistical analysis of the differences in the fracture resistances of the reinforcing materials, one-way analysis of variance (ANOVA) was performed using SPSS 21.0 (SPSS Inc., Chicago, IL, USA). When a significant difference was found, the Scheffé method was used for post-hoc testing (α = .05).
RESULTS
The weights of the constructed metal mesh and glass fiber mesh reinforcements, as well as those of the fabricated complete dentures with or without the reinforcements, are listed in Table 2. Because of the light weight of glass fiber mesh, the fiber mesh-reinforced denture was lighter than the metal mesh-reinforced denture and only 0.86 g heavier than the control group.
Among the 45 complete dentures (R, M, and F groups; n = 15 per group) that underwent fatigue testing, cracking or failure was not observed after cyclic loading.
Regarding fracture resistance (Table 3), the descending order was the metal mesh-reinforced, glass fiber mesh-reinforced, and unreinforced control groups, showing statistical significance (P < .05).
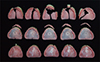
When the failure modes were analyzed in the results from the fracture resistance testing, striking differences in failure patterns were observed between the different reinforcing materials (Fig. 4). The failure mode of each specimen is listed in Table 4.
In the control group, cracks occurred, followed by complete fracture; all dentures were broken into multiple pieces of different sizes. However, none of the reinforced dentures showed complete fracture. In the metal mesh-reinforced complete dentures, cracks appeared in the acrylic resin and progressed further, while the posterior of the metal mesh was primarily fractured. Notably, all metal mesh frameworks were deformed by the ball-type jig, showing increased fracture resistance. Mostly after the complete fracture (81%) of the labial flange of the metal framework, fracture resistance was decreased. In the glass fiber mesh-reinforced complete denture, the posterior of the fiber mesh was both ripped and fractured (59.1%), but the shape of the denture was mostly maintained because the fibers were unbroken.
The results from fractography, performed with SEM, showed no evidence of fatigue failure, including fatigue striation, in any specimen. In the control group, a river line pattern was observed, in which several failure lines perpendicular to the polished surface were converging toward the tissue surface (Fig. 5).
On the fractured surface of the metal mesh-reinforced denture, a rough, complex pattern was seen, caused by static failure, while horizontal cracks along the plane of the metal mesh framework were observed in the resin base (Fig. 6A). A gap between the metal mesh and acrylic resin could be more clearly observed at a high magnification, and a river line pattern was also observed on the resin base (Fig. 6B). In the photograph taken at a magnification of 1,000×, the coexistence of concave dimple factures and convex interdendritic fractures was observed. A molten phase with a low melting point in a small round shape was also observed around the casting shrinkage cavity on the lower left; this does not grow, but sticks to the dendrites (Fig. 6C).
In the fiber mesh-reinforced denture, a broom-like failure was observed, occurring as crisscrossed fiber clumps broke (Fig. 7A). Mostly, crisscrossed spacing was observed, in which the glass fibers were separated from the acrylic resin, but fracture within the acrylic resin was also observed where the resin base and the glass fibers were bonded strongly (Fig. 7B). A higher magnification of this region showed that the glass fibers inserted into the resin matrix had fractures at different locations (Fig. 7C). Cracks within the glass fibers were observed, confirming a pattern in which the glass fibers were cleanly removed from the resin matrix (Fig. 7D). In addition, a radial pattern, as well as a microflow pattern on the resin surface, occurred on the fractured ends of the glass fibers (Fig. 7E).
DISCUSSION
During fatigue testing, the unreinforced control group showed bending when loading was applied, whereas the reinforced complete dentures did not show visible changes. The reinforced groups did not bend because the elastic moduli of the metal mesh and fiber mesh are higher than that of the resin denture base. Therefore, the metal or fiber mesh causes less damage to the denture-supporting tissues, because the fiber mesh-reinforced or metal mesh-reinforced denture is deformed relatively less during actual mastication.
Cracks or failures were not observed for any groups after fatigue testing, which may be because the fatigue loading of 80 N was too low or 300,000 fatigue loading cycles were insufficient to cause fatigue failure.
Vertical loading of 80 N was used in this study, so the loading delivered to the premolar on one side was approximately 40 N. This loading is similar to the chewing force on one side in patients with maxillary and mandibular complete dentures, as reported in previous studies1112 on occlusal force. The fatigue loading was applied 300,000 times, which is equivalent to using a complete denture for between 3 and 10 months.1314
Therefore, the results of the fatigue experiment in the study suggest that, when a patient uses maxillary and mandibular complete dentures, the fit of the denture to the denture-supporting tissues is deteriorated. With mastication at a normal chewing force for approximately 3 - 10 months, problems of cracking or failure may not occur. However, the mechanical strength can be decreased, regardless of the reinforcement material of the denture.
Regarding fracture resistance, significant differences were observed among the metal mesh-reinforced, fiber mesh-reinforced, and control group complete dentures. Differences were also observed in fracture progression for each type of complete denture. A ball-type jig was used, based on the previous research,67 for the fracture resistance tests. However, Yu et al.6 reported that the fracture resistance of the fiber mesh group was significantly higher than that of Cu–Zn metal mesh groups. In their study, the commercial metal mesh was hammered to form the shape on an edentulous cast. It was thinner (0.3 mm) and present at a lower volume percent than SES glass fiber mesh. In this study, the fracture resistance of the cast Cr–Co mesh-reinforced group showed an increasing trend because of a delay in fracturing caused by the deformation of the mesh. The fiber mesh-reinforced complete denture maintained its shape better than both the metal mesh-reinforced and unreinforced control-group complete dentures. This indicates that the fiber mesh-reinforced complete denture would be easier to repair because it would clinically maintain its shape to some degree even when damaged.
Praveen et al.15 reported the static fracture morphology of an acrylic resin denture base, which showed a few undercuts and generally clear surfaces. In this study, similar features were observed in the fractured surface of the resin base.
In Figure 5b, the direction of the river line pattern indicates the direction of the fracture proceeding from the polished surface toward the tissue surface. The vertical loading applied to the tissue surface of the palate may cause tensile force in the polished surface. Therefore, the crack in the acrylic resin begins and progresses from the polished surface toward the tissue surface, identical to the direction of fracture progression suggested by the river line pattern. Additionally, the posterior facing of the scarp indicates the horizontal progression of the fracture from the posterior border toward an anterior part.16 Thus, it can be inferred that fracture progressed from the polished surface of the posterior border toward the anterior tissue surface.
In Figure 6C of the Cr-Co metal mesh, the regular line pattern formed at approximately 90° are notable. The line pattern may reflect a fracture pattern of dendrites or dendrite arms. Dharmar et al.17 observed a similar pattern in the dendrites from a Cr-Co alloy of a different composition from that used in this study.
The SEM view of the fractured fiber mesh-reinforced denture (Fig. 7E) shows characteristic radials on the ends of the fibers and a microflow pattern on the resin surface. By examining the radials and microflows, the directions of local crack growth can be inferred. The fiber fracture started at the initiation site, from which the radials fanned out. Therefore, it can be inferred that the fracture first occurred in fiber A and then progressed through the neighboring areas in the resin matrix to fibers B, C, and D, in order.
Figure 7A and 7B showed a large gap between the fiber mesh and acrylic resin. If water were to enter the gaps caused by denture failure in the oral environment, the strength of the resin would be reduced, and interfacial debonding would be accelerated because the surface of the glass fibers would be attacked and the silane coupling agents would undergo hydrolysis.918 Therefore, a lower degree of cohesion between the glass fiber and resin matrix would cause faster strength deterioration when crack was to occur in fiber mesh-reinforced dentures.
In addition, a broom-like failure pattern was observed, in which the broken fibers had different lengths. This is different from the cleanly fractured surfaces shown on specimen fracture in other studies.89 This is because these studies used a glass fiber bundle product with a lower ratio of glass fiber per area compared to the glass fiber mesh used in this study.
In the present study, the fiber mesh-reinforced complete denture showed a higher fracture resistance than the control group. It was also lighter, more aesthetically pleasing, and quicker to process than the metal mesh-reinforced complete denture. Even after fracture occurred, the structure of the fiber mesh-reinforced complete denture was maintained, indicating that it could be easier to repair. The metal mesh-reinforced complete denture exhibited a higher level of fracture resistance compared to the fiber mesh-reinforced denture, but the impact from the deformation of the metal mesh was large. Based on studies like the present one, the long-term stability of fiber mesh- and metal mesh-reinforced complete dentures can be confirmed through follow-up clinical studies on their survival rates. If the volume percentage of the reinforcement were calculated, the reinforcements could be compared regarding mechanical properties.
Midline fracture is a common problem in complete dentures, so fatigue loading in a water bath is generally used to reproduce midline flection.910 However, with the T-bar only applied to the second premolar on each side, the loading is different from clinical masticatory conditions. In the fracture resistance test, the load was applied only on the palatal area of the denture to obtain static fracture in the midline area. Because of this, the large deformation of the Cr–Co metal mesh had a significant effect on the fracture resistance, which differed from the behavior of the fiber mesh. The fracture test loading scheme also differs from clinical conditions.
In future studies on denture reinforcement materials, it would be prudent to consider these limitations and compare dentures under conditions similar to clinical conditions.
CONCLUSION
Under certain limitations, this study examined the effects of different reinforcing materials on the fracture resistances of dentures by using fatigue loading and fracture resistance tests. None of the maxillary complete dentures showed cracks or fractures, even after 300,000 cycles of fatigue loading. The descending order of fracture resistance was the Cr-Co alloy metal mesh-reinforced complete denture, glass fiber mesh-reinforced complete denture, and unreinforced complete denture, and the differences among the failure modes of the three types were significant. The metal mesh-reinforced complete denture broke mostly by fracturing in the posterior border, and showed a high fracture resistance because of the deformation of the all-metal mesh. In contrast, the glass fiber mesh-reinforced complete denture largely maintained its original structure even after fracturing because of the unbroken fibers.










 XML Download
XML Download