

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In dentistry, dental zirconia is widely used for fabrication of restorations.1 In the past, it was generally used as substructure for supporting veneering porcelain. However, in recent years, monolithic zirconia has been commonly used for fabrication of dental prosthesis, ranging from a single crown to full arch restoration.2 Owing to the high strength of monolithic zirconia, it overcomes the fracture or chipping problems associated with veneering porcelain.3 Monolithic zirconia with increased translucency has also been developed for use in esthetic regions.4
Dental ceramic materials for esthetic restorations have been under continuous development and are increasingly used in different treatments. In contrast, the frequency of use of dental alloys, such as gold alloys, Ni-Cr, and Co-Cr alloys, has decreased in recent times, but the alloys remain necessary and are effective because of their high modulus of elasticity and hardness, corrosion resistance, and low cost.5 Occasionally, base metal alloys and zirconia prostheses can be located in opposite positions during mastication; clinicians should consider the possibility of wear between the metal restoration and the zirconia prosthesis in such cases when establishing a treatment plan.
Monolithic zirconia has a relatively high surface hardness compared to that of other dental restoration materials. Many studies have reported the wear of enamel and other restoration materials opposed by monolithic zirconia. Most in vitro studies have reported that monolithic zirconia showed similar or less enamel wear than that induced by feldspathic porcelain.6789 In clinical trials, monolithic zirconia showed greater enamel wear than that induced by natural teeth.1011 Most of these articles were concerned with wear between monolithic zirconia and enamel or dental ceramics; however, little has been reported about wear between monolithic zirconia restoration and base metal alloy restoration, such as Ni-Cr or Co-Cr alloys.
Here, we report on a case with a surface metal stain on a monolithic zirconia restoration that opposed a restoration made from a base metal alloy.
CASE REPORT
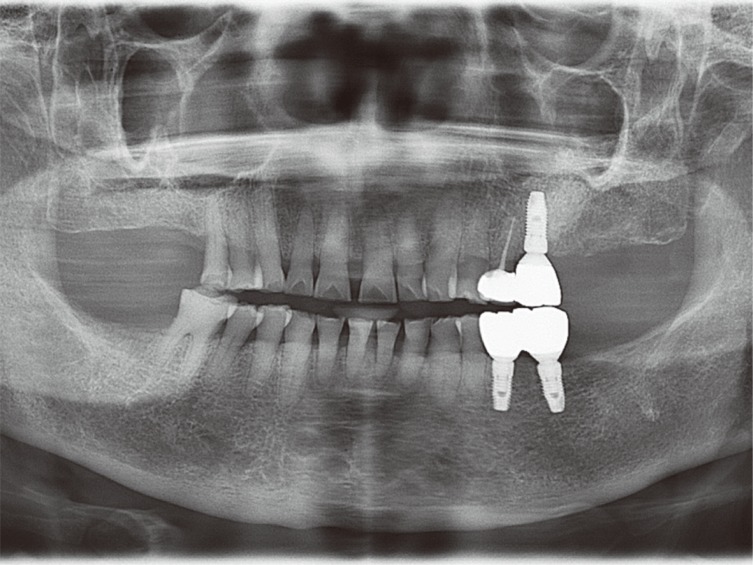
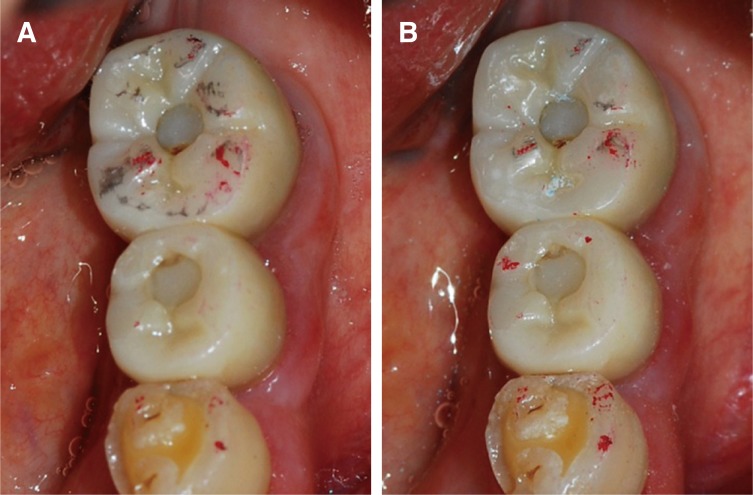
A 71-year-old woman visited our clinic with a complaint of black stains on left mandibular first molar, which had been treated with implant-supported fixed partial prostheses. During that visit, 14 months prior to attending clinic, the patient had presented with loss of multiple teeth; right maxillary first and second molars, left maxillary second molar, right mandibular second molar, left mandibular second premolar, left mandibular first and second molars were missing. On the left maxillary second premolar, the patient had a porcelain-fused-to-metal crown with a porcelain occlusal surface, and a porcelain-fused-to-metal crown with a metal occlusal surface were restored on the left maxillary first molar. Owing to financial constraints, the right-side molar region and left-side second molars were not included in the treatment plan. Left mandibular second premolar and left mandibular first molar were treated with implant-supported fixed partial prostheses, using monolithic zirconia (Prettau, Zirkonzhan GmbH, Bruneck, Italy). 6 months later, she complained about the stain (Fig. 1, Fig. 2).
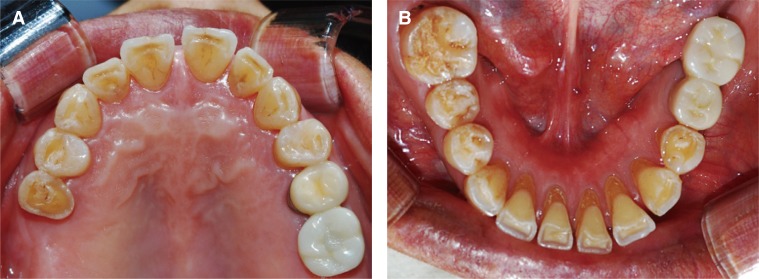
The patient had an unstable maximum intercuspal position, and occlusal pattern was a nearly bilateral balanced occlusion (BBO) (Fig. 2A). Black stains were observed on the occlusal surface of the left mandibular first molar (Fig. 2C). Upon visual clinical examination, insufficiently polished occlusal surfaces were detected on the monolithic zirconia restorations of the left mandibular second premolar and left mandibular first molar. At the time, the rough occlusal surfaces of the monolithic zirconia and occlusal interference during lateral movement of the mandible were considered as the main causes of the stain. Therefore, surface polishing of restorations and occlusal adjustment were performed (Fig. 3).
However, 3 months after the polishing, the black stains remained on the same surfaces. To resolve this problem, the final restoration made from monolithic zirconia on the left mandibular first molar was removed, and a provisional restoration made from acrylic resin (ALIKE, GC, Tokyo, Japan) was placed instead. A month later, the black stain was not observed on the occlusal surface of the provisional restoration.
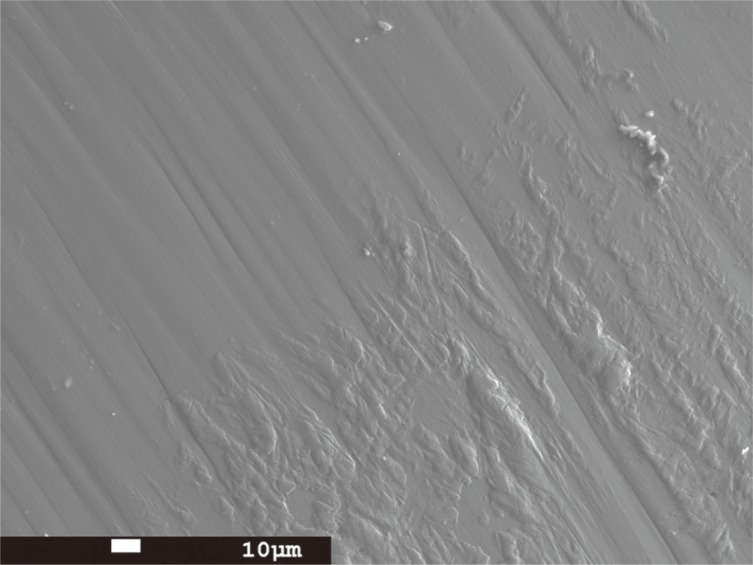
To determine the cause of the stain, surface roughness measurement (Ra) and electron probe micro-analysis (EPMA) were performed on the removed monolithic zirconia restoration. A profilometric contact surface measurement device (TR-200, Beijing TIME High Technology, Beijing, China) was used to measure the surface roughness. Four measurements were made on an unstained portion on the surface of the removed monolithic zirconia prosthesis adjacent to the stained area (length: 0.25 × 1 mm, range: 40 µm, standard ISO), and the mean surface roughness was Ra = 0.209 µm (SD 0.019).
The base metal alloy used for the prosthesis of left maxillary first molar was Ni-Cr alloy (ARGELOY N.P. STAR, Argen, San Diego, CA, USA), which contained Ni, Cr, Mo, and Si as its main components (metal content, in %: Ni 61.2, Cr 25.8, Mo 11, and Si 1.5). The monolithic zirconia used for the restoration of the left mandibular first molar contained Zr and O as its main components. To analyze the stained surface on the monolithic zirconia restoration of the patient's left mandibular first molar, an electron probe micro-analyzer (JXA-8530F, JEOL, Tokyo, Japan) was used to detect Zr, O, and the 4 elements of the Ni-Cr alloy. The secondary electron image on the occlusal surface of the removed monolithic zirconia prosthesis revealed the presence of foreign material in the lower right region (Fig. 4). In the area of the foreign material, mostly Ni, Cr, Mo, and Si were detected, while, in the upper left region, mainly Zr and O were detected (Fig. 5). This indicated that the black stain was in fact a metal stain originating from the Ni-Cr alloy material that was used for the restoration of the left maxillary first molar, which had a metal occlusal surface. Thus, to eliminate the cause of the metal stain, the Ni-Cr alloy restoration was replaced with monolithic zirconia restoration. By 3 months after this replacement, the black stain on the occlusal surface of monolithic zirconia restoration of the left maxillary first molar was no longer observed (Fig. 6).
DISCUSSION
The occlusal adjustment of restoration is an essential chairside process but induces changes in surface roughness. A rough or smooth surface resulting from the polishing procedure after in-clinic occlusal adjustment can influence the amount of wear on the opposing antagonist.12 In previous studies related to the wear aspects associated with surface roughness of monolithic zirconia,679131415 the range of surface roughness of polished monolithic zirconia is known to be 0.04 - 1.11 µm and zirconia with a smooth surface generally induces less wear on the opposing specimen than zirconia with a rough surface. In this present case, the measured surface roughness (Ra) of zirconia was 0.21 µm. Since this value fell within the range of values given in the aforementioned studies, zirconia restoration was thought to have been adequately polished. The roughness of the zirconia restoration in the present case was clinically acceptable because this value approached the threshold surface roughness for bacterial retention (0.2 µm).16
Kanbara et al.17 previously reported a similar surface stain on zirconia, caused by wear between a titanium alloy and a highly polished zirconia (Ra < 0.1 µm). Although their study dealt with a different alloy, their finding implies that the black metal stain found in the present case report was unrelated to the surface roughness of monolithic zirconia restoration.
Koran et al.18 stated that a high load and sliding speed during mastication increases the coefficient of friction, inducing greater wear. The restoration in the present case was located in molar area, which has a high chewing force, and an occlusal pattern close to a BBO may have induced the exertion of force accompanied by sliding movement. Moreover, the missing right maxillary first molar, right maxillary second molar, and right mandibular second molar may have compelled the patient to employ unilateral mastication on the left side, which may have concentrated the occlusal force on the left side. These factors could have induced severe wear of the metal occlusal surface on the left maxillary first molar, and this phenomenon was thought to be the major cause of the stain on the monolithic zirconia.
Wear of dental ceramics other than monolithic zirconia against enamel or dental ceramic does not occur by plastic deformation, but by fracture, and the surface hardness of the restorative material alone is not a reliable predictor of the wear of brittle materials.19 However, an in vitro study on wear between titanium alloy and zirconia20 has reported that the amount of wear of titanium alloy opposing zirconia was 20 times higher than that of the zirconia, and pointed out that this is due to the hardness of zirconia. In addition, a previous study20 has also described that, while adhesive wear occurred between metal and metal, abrasive wear occurred between zirconia and metal. In the present case, a secondary electron image revealed the presence of Ni-Cr alloy as a foreign body on the zirconia surface (Fig. 5). This suggests that the early stage in the wear between monolithic zirconia and Ni-Cr alloy could have occurred as abrasive wear, but as wear progressed to a certain level, adhesive wear could also have occurred by interaction between metal on the zirconia restoration surface and the metal of the opposing Ni-Cr alloy antagonist tooth restoration, triggering a combination of both wear mechanisms.
Many restorations previously made from various metal alloys may already exist in the patients' oral cavity. However, some studies about wear between zirconia and gold alloy have been reported,15 and there are few reports about wear between zirconia and base metal alloy. Thus, further in vitro and/or in vivo studies about wear between monolithic zirconia and various dental alloys are needed.
In conclusion, the surface of a monolithic zirconia restoration could be stained by wear of the opposing Ni-Cr alloy prosthesis; dentists should consider this when choosing restoration materials.


 XML Download
XML Download