

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In order to satisfy the high esthetic needs in the maxillary anterior region, it is crucial that there be a harmonious relationship between the teeth and the surrounding soft tissues.12 However, alveolar ridge defects caused by trauma, tooth extractions, advanced periodontal disease, etc. lead to unnatural emergence profile and prolonged clinical crown length of maxillary anterior prosthesis. Hence, improvement of the localized alveolar ridge defect is vital in enhancing the esthetics of fixed partial denture, especially in the maxillary appearance zone.3
Reconstructive techniques to augment the deformed alveolar ridge can be classified in two groups based on their coverage degree: soft tissue graft and hard tissue graft.4 In general, soft tissue graft is widely used to get the natural emergence profile of pontics due to short healing period, more predictable result, and simple procedure. Studer et al.5 described types of soft tissue augmentation as follows: 1) the roll flap technique6 and modifications,7 the onlay transplant technique89 and modifications10 and 3) the subepithelial connective tissue transplant technique11 and modifications.12
Roll flap technique6 involves a de-epithelialized connective tissue pedicle flap. Advantages of this technique include maintaining the color and texture of the patient's soft tissue, and requiring only single operative site. However, this technique is recommended only for the Seibert Class I defect of mild severity due to limited supply of donor tissue. Combination onlay-interpositional graft13 is a technique that is utilized mainly for buccolingual augmentation by inserting the de-epithelialized portion of graft into labial pouch of deformed ridge and could be also used for apicocoronal augmentation if the epithelialized section of transplant is positioned above the surface of the tissue surrounding the recipient site. It is consequently recommended for Seibert Class I, III ridge defect.
A common problem of the connective tissue graft for alveolar ridge defect is that it requires multiple operations due to insufficient volume of donor tissue to reconstruct the alveolar ridge defect to its original dimension.6
One of the alternatives to overcome this limit might be a technique that combines two types of soft tissue augmentation techniques, several of which have been reported. Seibert and Louis13 presented a combination onlay-interpositional graft procedure as predictable soft tissue ridge augmentation in class III ridge defect. Stimmelmayr et al.14 reported a combination epithelized-subepithelial connective tissue graft for closure and soft tissue augmentation of extraction site.
The purpose of this paper was to describe the new combined technique of roll flap and combination onlay-interpositional graft utilized to get sufficient dimension and contour of recipient area by one time of operation and to present the esthetic improvement such as the natural-looking emergence profile of fixed partial denture in case of localized maxillary anterior ridge defect.
CASE REPORT
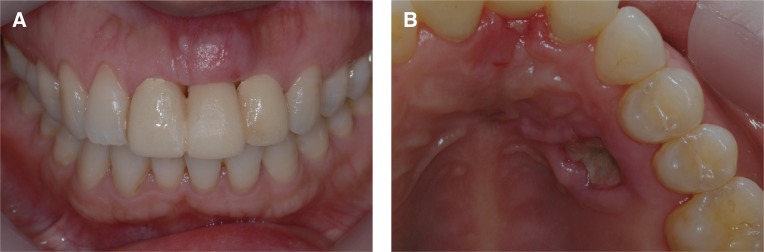
A 40-year-old female presented with a chief complaint of the inconvenience and unesthetic problem of maxillary anterior prosthesis due to the space between pontic and underlying gingiva, the cocave gingival contour above pontic, and the color disharmony.
#21 tooth was extracted about 10 years ago and it was recovered by 3-unit (#11=#22) ceramo-metal restoration. Because of ridge resorption, edentulous area occurred about 2.0 mm space between pontic and gingiva. So inconveniences such as food residue and reduced esthetics were predicted (Fig. 1).
After removal of old prosthesis, intraoral examination revealed moderate (buccolingually 4mm) ridge deficiency in missing tooth region, leading to the diagnosis of Class I alveolar ridge defect (Fig. 2). Seibert8 classified the localized ridge defect as Class I : horizontal or buccal tissue loss with normal ridge height, Class II: vertical or apicocoronal tissue loss with normal ridge width, and Class III: combined horizontal and vertical bone loss. Allen et al.15 reported the classification of soft tissue defect as minor when less than 3 mm, moderate when 3 to 6 mm, and extensive when greater than 6 mm.
By considering bone level of adjacent teeth and donor site condition, the surgery plan was established to use the combined technique of roll flap and interpositional graft procedure to maximize ridge augmentation and reduce the number of surgery.
The area subjected to surgery was anesthetized by infiltration anesthesia using 2% Lidocaine with 1:100,000 epinephrine. After administering disinfection and local anesthesia, a partial-thickness crestal incision was made mesiodistally at the height of ridge, and was continued as sulcular incision to the distolabial surfaces of the abutment teeth. On palatal side of the ridge, the gingival surface was de-epithelialized in a trapezoid and the full-thickness rectangular pedicle with de-epithelialized connective tissue was made by a No. 15 scalpel blade. The subperiosteal soft tissue pocket was created on the labial surface of the deformed ridge. The de-epithelialized connective tissue pedicle raised from palate using sharp dissection was rolled and placed in this pocket (Fig. 3).
After Roll procedure was completed, the donor site was prepared on the premolar palatal area of the maxillary left side for combination onlay-interpositional graft. The trapezoidal shaped transplant was made of the de-epithelialized and epithelialized part. The de-epithelialized connective tissue region of the graft was inserted into the pouch created within the deformed ridge. In order to position and immobilize this segment without any contact and subsequent delay, the transplant was immediately fixed with two separate suture materials prepared in advance on both ends of the bottom of the pouch. The epithelialized section of the graft was positioned above the surface of the surrounding tissue at the crest of the ridge. Since the viability of soft tissue graft is dependent on tight adaptation, immobility, and immediate transplantation for healing, the operator paid particular attention to this procedure (Fig. 4). Sugicel was placed into the palatal wound to control hemorrhage after multiple suturing.
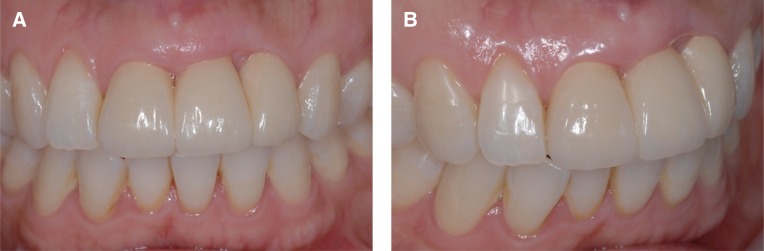
After the suturing had been completed, provisional prosthesis with ovate pontic was directly modified and placed in position (Fig. 5). It was estimated that immediate placement of this provisional restoration would contribute to getting optimal ovate seat and desired labial relationship for natural emergence profile of fixed partial denture with lesser volume of graft soft tissue by supporting the tissue from inside. The sutures were removed at 1 week post-surgery after good healing state of operation site was checked (Fig. 6). Healing in the recipient site had matured considerably by 6 weeks post-surgery. The final fixed partial denture was delivered at 7 weeks post-surgery (Fig. 7). This prosthesis has been observed natural-looking emergence profile and stable alveolar ridge until about 18 months after the surgery (Fig. 8).
DISCUSSION
The deformation in the alveolar ridge is related to loss of root structure and alveolar bone damaged by trauma or periodontal disease. Although there is no precise criteria to select the soft tissue graft or hard tissue graft up to date, the extent of alveolar ridge defect, the state of donor site, and whether installation of implant or not etc. should be comprehensively considered for ridge augmentation.15
In addition, the estimation of healing period and amount of atrophy expected after grafting is required. Perenack et al.16 reported that most atrophy occurred within the first 6 weeks after performing subepithelial connective tissue graft and about 40% of graft underwent contraction. Therefore, when conducting soft tissue augmentation, the size of the recipient tissue should be increased by 120-150%. Oliver et al.17 mentioned that the healing of the free soft tissue graft took about 2 months through the periods of initial stage, revascularization, and tissue maturity stage. Studer et al.5 reported that the definitive impression for final prosthesis should be taken at least 3, preferably 4, months postoperatively. Wiskott18 mentioned that healing period of 6, preferably 8, months before proceeding with final restoration was necessary.
In this case, however, although final restoration was delivered at 7 weeks post-surgery, the natural-looking prosthesis with optimal emergence profile and contour was obtained and possible reasons are summarized as follows: 1) the transplant was immediately placed without any contact and subsequent delay such as removing fat layer or trimming graft on the glass plate after taking the graft. 2) The transplant was quickly stabilized and tightly adapted into position with two separate sutures prepared on both sides of the bottom of the pouch. 3) The provisional prosthesis with ovate pontic was promptly placed to get optimal ovate seat and to support the soft tissue from inside for the desired labial relationship of fixed partial denture.
Unfortunately desired contour of the interdental papilla between maxillary left central incisor and maxillary left lateral incisor was not optically recovered in this case. This was predicted to be a result of the inadequate flap design that the interdental papilla adjacent to the maxillary left lateral incisor was not completely included within the flap. Therefore, it cannot be emphasized enough that there be an accurate flap design for a successful soft tissue ridge augmentation.
This combined technique might be significant as a new improved technique utilizing the roll flap and combination of onlay-interpositional graft to reduce the time of surgery and to get more predictable esthetic results of fixed partial denture in cases of maxillary anterior localized ridge defect.






 XML Download
XML Download