

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Radiotherapy is widely used to treat head and neck cancer, as a primary therapy, adjuvant to surgery, or as a palliative treatment for unresectable head and neck malignancies. In cases of oral and maxillofacial tumors, oral functions and esthetics are often compromised after resective surgeries, which require rehabilitation procedure. Especially, dental rehabilitation is often more complicated by anatomical changes due to tumor resection and reconstruction, with a decreased area of attached mucosa and limited movement of the tongue being the most frequently encountered problems.1 Trauma induced by removable prosthetic appliances for edentulous area might cause injury to oral mucosa and alveolar bone and be considered as a predisposing factor of osteoradionecrosis.2 Therefore, although radiation impairs the vitality of skeletal tissue, rehabilitation with oral implants is considered as a valuable treatment option since they can minimize the trauma induced by removable prosthetic appliances.
Oral reconstruction using dental implants in head and neck cancer patients has focused mainly on implant placement after radiotherapy because (1) implant placement during ablative surgery requires a thorough presurgical examination and multidisciplinary consultation for well-established treatment planning, (2) the excision border may enlarge during surgery, and (3) (sometimes) because second surgery for reconstruction is planned. In addition, the vascularization and regenerative capacity of the irradiated tissues can be decreased after radiotherapy, and this may have a negative effect on the osseointegration of the dental implants. Surgical intervention in irradiated bone is also thought to increase the risk of osteoradionecrosis.
Therefore, some authors have advocated the opposite strategy of implant placement before radiotherapy (post-implant radiotherapy).34 The main advantages of this post-implant radiotherapy in the literature are as follows456:
Avoidance of a second surgical intervention, which is a major advantage considering the psychological and physiological exhaustion caused by tumor treatment that can discourage patients from undergoing a second surgical intervention.
Initial implant healing can be achieved before irradiation.
Implant surgery in compromised area by radiotherapy is avoided, thus reducing the risk of late complications or osteoradionecrosis.
Prosthetic reconstruction and rehabilitation can start early, providing the patient with a more timely improvement in oral function, which is important for the rehabilitation of speech and swallowing.
It is currently unknown whether post-implant radiotherapy has a negative effect on the survival of implants located in the radiation field. Few studies have addressed treatment outcomes of implants for post-implant radiotherapy procedure. There have been a few animal studies of the post-implant radiotherapy after implant surgery in maxillae or mandibles,7891011 but only one of these focused on the effect during the early stage of the healing. The purpose of study was to elucidate the biologic effects of post-implant radiotherapy (1 day or 4 weeks after implant placement) on the osseointegration of the implants during the 2, 4, and 8-week healing.
MATERIALS AND METHODS
Forty-eight Sprague-Dawley rats (4-week-old males with body weights of 130 - 140 g) were divided into a radiation (exp.) group (n = 24) and a non-radiation (control) group (n = 24). Each group had three subgroups according to the healing time between implant placement and sacrifice; 2, 4, and 8 weeks. The exp. group 1, and 2 received radiation 1 day after implant placement. The exp. group 3 received radiation 4 weeks after implant placement.(Table 1) These intervals for the experiments followed the protocol of one previous study which showed establishment of osseointegration 28 days after implant placement.12
All necessary surgical procedures were conducted under general anesthesia via the intraperitoneal injection of an anesthetic cocktail composed of Rompun (xylazine, 20 mg/mL, 0.5 mL/kg body weight; Bayer, Leverkusen, Germany) and Zoletil (tiletamine and zolazepam, 100 mg/mL, 0.5 mL/kg body mass; Virbac Laboratories, Carros, France).13 Both maxillary first molars of all animals were extracted. At 4 weeks after tooth extraction, a small, full-thickness flap was elevated at each recipient site. A 1.5-mm-deep implantation osteotomy was prepared with a low-speed, diameter (Ø) 1.0-mm round bur and subsequently a Ø1.3-mm fissure bur and a Ø1.45-mm twist drill. Customized sterile, grade IV titanium implants (Ø1.5 × 2.5 mm) were inserted bilaterally into the drilled cavities using a hand driver and tapped with a mallet so that their tops were situated just at the cortical bone surface, or roughly 0.5 mm below the bone (Fig. 1). The flaps were then repositioned carefully without suturing. After surgery, the rats were housed with free access to food pellets and tap water. The rats were allowed to survive for 2 weeks (exp. and control group 1), 4 weeks (exp. and control group 2), or 8 weeks (exp. and control group 3) after implant placement.
Fluorescence expression agents were injected intraperitoneally into the rats to enable observation of specimens from these animals under a fluorescence microscope, as follows: oxytetracyclineHCl (oxy-TC, yellow; Pfizer, Seoul, Korea; 20 mg/kg) was injected on the same day as implantation, calcein green (Sigma, Tokyo, Japan; 20 mg/kg) was injected 2 weeks later (1 week later for exp. and control group 1), oxy-TC at 4 weeks later in exp. and control group 3, and alizarin-3-mothylinimodiacetic acid (alizarin red S; Sigma, Tokyo, Japan, 20 mg/kg) was injected 1 day before sacrifice.
On the day of being killed, the rats were perfused transcardially with 4% paraformaldehyde while under general anesthesia. Then their maxillae, including the implants, were removed en bloc and immersed in the same fixative for an additional 24 hours.
Radiation groups were irradiated according to the experimental schedule while under general anesthesia. They were immobilized in a customized fixation device and the radiation fields were verified using an external beam simulator (Nucletron, Veenendaal, The Netherlands). The rats received localized radiation with a single, 15.0-Gy dose to the maxilla using a 6.0-MV linear accelerator (Elekta, Stockholm, Sweden), which is commonly used to administer radiation treatment in humans. This is biologically equivalent to 55 Gy delivered in 25 sessions of 1.8 Gy each five times per week within a 5-week period.14 The treatment focus was located at the midpoint between the first molars of the maxilla, and a field size of 2 × 2 cm was used to irradiate the implant site and surrounding bone tissue (Fig. 2). Radiation was delivered with parallel-opposed lateral fields at a dose rate of 4.19 Gy/min.
Before decalcification of the specimen, a three-dimensional (3D) microcomputed tomography (micro-CT) image was taken for each rat using a micro-CT scanner (Polaris-G90, NanoFocus Ray, Kwangju, Korea) at 50 kV and 180 mA. This was reconstructed using OnDemand 3D software (Cybermed, Seoul, Korea) to obtain volumetric information and the relative bone mineral density (BMD) in the proximity of the implants.
After completing micro-CT, all specimens except for one from each group were decalcified with 10% EDTA at 4℃ for 1 month. The decalcified specimens were first embedded in paraffin wax using a standard protocol, and then a series of 7-µm-thick sections were prepared. The specimens were stained with hematoxylin-and-eosin (H&E) stain. The stained specimens were observed with a light microscope (DM 2500, Leica Microsystems, Wetzlar, Germany).
Bone-to-implant contact (BIC) was measured at the distal surface of the implant, and empty lacunae were counted in the region of interest (ROI) for the quantification of necrotic bone using IMT i-Solution lite ver. 8.1 software (IMT i-Solution, Vancouver, BC, Canada). Bone area was measured in the same ROI. According to previously reported papers, injured pre-existing bone is usually located within 100 - 500 µm beyond the bone cavity margin.1215 In the present study, the width of the peri-implant ROI was set as 300 µm from the surface of the implant, as advocated by Kim et al..16
One specimen from each group was fixed with 10% neutral buffered formalin (pH 7.0) for 2 weeks, and then dehydrated with ethanol and embedded in methylmethacrylate (Technovit 720VLC, Heraeus Kulzer, Dormagen, Germany). The specimen was cut along the center axis of the implant with a cutting system (Exakt 300, Kulzer, Norderstedt, Germany). The central section of each specimen was cut to a thickness of 15 µm using a microgrinding system (ExaktApparatebau, Norderstedt, Germany). The sectioned specimens were dyed with H&E and observed under an optical microscope and a fluorescence microscope (DM 2500, Leica Microsystems).
According to the test of normality, nonparametric and parametric statistical analyses were implemented. The data about BMD conformed to a normal distribution, the mean differences were verified with the independent two-sample t-test and analysis of variance (one-way ANOVA).The level of statistical significance was set at 5% (i.e., P < .05). Other data did not conform to a normal distribution, they were evaluated using Wilcoxon rank-sum and Kruskal-Wallis tests. The Bonferroni test and Dunn's test were used for post-hoc multiple tests. All calculations were performed using a standard statistical program (SAS for Windows, version 9.2; SAS, Cary, NC, USA).
RESULTS
Among the initial cohort of 48 rats, 4 rats died unintentionally during the study and 18 implants were lost from the remaining 38 rats (Table 2).
The implants were partially surrounded by trabecular bone. BMD differed significantly between the control and experimental groups. When comparing the nonirradiated groups, BMD increased with the length of the healing period. BMD was significantly lower in exp. group 1 and 2 (which were irradiated during the early healing stage) than in the corresponding control group 1 and 2. BMD of exp. group 3 (irradiation during the late healing stage) was similar to that of control group 3 (Fig. 3).
BIC gradually increased with the healing period, but the differences were not statistically significant. BIC was lower in the exp. groups than control groups, but the large amount of variation among the data meant that the differences did not reach significance. The bone volume fraction (i.e., bone volume/tissue volume) gradually increased with the healing period. Comparison of the exp. group with control groups revealed that the bone volume was lower in the exp. 2, and 3 groups than the control 2, and 3 groups (P < .05). The empty lacuna count (i.e., empty lacuna/bone volume) did not differ between the control groups; empty lacunae remained 8 weeks after implant placement. In the irradiated groups, the empty lacuna count was higher in exp. groups 2 and 3 than exp. group 1. Significant differences between exp. and control group 2 (P < .10) and between exp. and control group 3 (P < .05) was found. Empty lacuna count was higher in the exp. 2, and 3 groups than other groups (Fig. 4).
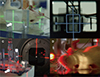
Active bone-forming areas were observed via fluorescence analysis. When viewed through the green filter (wavelength, 515 - 560 nm), oxy-TC and calcein green emitted yellow and green light, respectively, while alizarin red S emitted red light when viewed through the red filter (450 - 490 nm).
Among those animals sacrificed at 2 weeks after implant placement, there was more bright red fluorescence than green fluorescence, indicating an acceleration of new bone formation. Red fluorescence appeared at the implant interface in those animals sacrificed at 4 weeks after implant placement, while green and red fluorescence appeared at the border of the old bone in those sacrificed at 8 weeks after implant placement (Fig. 5).
DISCUSSION
Implant placement prior to postoperative radiotherapy-preferably simultaneously with ablative surgery-not only obviates the need for additional surgical reconstructive surgery but also advances prosthetic reconstruction. In studies with dental implant placement after tumor therapy, the patients had to wait 17.0 - 44.5 months before the implants were placed, and a delayed rehabilitation period could start.171819 The clinical study of Schepers et al.1 found that the interval between the end of tumor therapy and the start of prosthetic rehabilitation was 4.8 months and a 97% success rate of osseointegration was reported for their post-implant irradiated group. In other clinical studies, although the samples were too small for statistical analysis, the reported success rate of implants before radiation was acceptable. The authors therefore recommended implant insertion during ablative surgery if postoperative radiotherapy is scheduled or possibly will be applied.56
Radiation injury to the fine vasculature of bone results in a further reduction of the number of cells and progressive fibrosis. The remodeling system of bone-comprising osteocytes, osteoblasts, and osteoclasts-is also damaged. Some osteocytic lacunae become empty, devoid of osteocytes.2021 Jacobsson et al.22 demonstrated that irradiation has an acutely negative effect on bone regeneration, reporting that regeneration activity was decreased by 70.9% during a 4-week period of irradiation in rabbits. That study found a significant depression of osteogenesis around implants when they were inserted immediately after irradiation. Significantly reduced bone-regenerative capability and reduced implant osseointegration in irradiated dog and human alveolar bone have also been reported.23 The sensitivity to irradiation is higher for immature bone than for mature bone.24 Clinically, postoperative radiation therapy is commonly initiated 14 - 21 days after ablative surgery,10 at which time wound healing is not yet complete. A reduced regenerative capacity in bone after irradiation in rabbits has been reported, and the contacting bone may fail to become lamellated within the normal time period, and may reduce the adherence to the implant surface at 4 weeks after irradiation with a single 15-Gy dose.10 The present study analyzed the relative BMD, BIC, bone volume, and empty lacuna count in order to evaluate the modeling and remodeling rate.
A recently developed technology allows the evaluation of bone biopsies with 3D micro-CT. The parameters computed by micro-CT were bone volume, bone surface, trabecular thickness, trabecular separation, bone connectivity, and bone-to-implant apposition. Data from micro-CT analysis are reported to be reliable, but the titanium implant was found to cause a blurred border of 45 - 60 µm along the implant surface.2526 This was affected by the difference in thickness between the titanium implants (2.0 mm and 3.5 mm), with the quality of the micro-CT image being influenced more by a thicker titanium implant. The present study used implants with a smaller diameter (1.5 mm) and measured BMD within 300 µm of the ROI. BMD is calculated by measuring Hounsfield units and relating those values to a calibration bone phantom with a predetermined BMD.27 However, an absolute BMD value based on CT scans is not possible without scanning calibration bone phantoms with predetermined BMD values.28 Therefore, in the present study, relative BMD-which is determined during CT scanning-was calculated.
It is considered that radiation damage is the most important factor leading to decreased bone matrix formation and disturbance of bone mineralization.29 Verdonck et al.28 compared BMD values in irradiated and nonirradiated groups of minipigs, and found that BMD was greater in the irradiated group than in the nonirradiated group at 3 months after irradiation, although the difference was not statistically significant. The authors assumed that irradiation had a negative effect on bone vascularity, and hence on bone sclerosis. In the present study, BMD was significantly lower in exp. groups during the early healing stage than the corresponding control groups. BMD was similar in exp. and control group 3 (irradiated during the late healing stageand the corresponding control group). When comparing the control groups, BMD increased with the length of the healing period. This indicates that irradiation during the early healing stage significantly decreases bone remodeling, while that administered during the late healing stage doesn't.
According to previous studies,1230 extraction socket healing takes 1 month in rats. There was new bone formation at 5 days after implantation. At 28 - 30 days post-implantation, the newly formed woven bone was almost completely in contact with the implant surface. The preexisting bone with empty osteocytic lacuna still remained in the area where the implants had been installed in close contact with the bone. Aitasalo29 reported that the decrease in the number of osteoblasts following irradiation decreased collagen production and increased the number of empty lacunae in the cortical bone. This increase was dose-related, since osteoblasts were destroyed after a radiation dose of 10 Gy.10 In animal studies, BIC was lower in the post-implant irradiated groups than in the non-irradiated groups with subjective observations showing retarded bone formation and peri-implant bone resorption.1011 Brogniez and colleagues have reported the effects of irradiation before and after implant placement in dog models.789 In contrast to earlier studies, they found that the bone-healing capacity was relatively unaffected by irradiation, and the BIC appeared to be better in those irradiated after implant placement than in those irradiated before implant placement. In our study, the BIC and bone volume gradually increased with the healing period, indicating that osseointegration takes 8 weeks or more in accordance with the findings from the study by Haga et al.31 Lower bone volume was found in irradiated group irrespective of the time point of irradiation (1 day or 4 week). This might indicate that irradiation affects bone healing during both the early and late stages of the osseointegration process.
The empty lacuna count did not differ significantly between the three control groups; empty lacunae still existed 8 weeks after implant placement. In the exp. groups, the empty lacuna count was higher in groups 2 and 3 than group 1, which is consistent with the findings of a previous study.29 In comparison between the exp. and control groups, significant differences were found between exp. and control group 2 (P < .10) and between exp. and control group 3 (P < .05). This indicates that bone healing after irradiation was retarded regardless of the stage of osseointegration, and it was also consistent in the result from the bone volume analysis.
In the fluorescence analysis, the bone mineral apposition patterns for the various healing periods were compared. The diameter of the Haversian systems is the most optimal and diagnostic measurement to use, but due to the poorly developed Haversian systems in rats and the small sample, only subjective observations were performed. In animals at 2 weeks after implant placement (exp. and control group 1), there was more bright red fluorescence than green fluorescence, indicating acceleration of new bone formation. These findings were in accordance with those from the study by Schön et al.10 New bone formation was accelerated at 12 - 19 days after implantation. At 4 weeks after implant placement (exp. and control group 2) in animals, red fluorescence appeared at the implant interface, which is also consistent with previous studies. At 8 weeks after implant placement (exp. and control group 3) in animals, green and red fluorescence appeared at the border of the old bone, indicating continuous bone remodeling. Comparison of the irradiated and nonirradiated groups revealed retarded new bone formation in the irradiated group.
One thing that should be considered when choosing radiotherapy after implant placement is the backscattering effect of the metal implants. There is no general agreement regarding the explantation or preservation of metal dental implants in patients subjected to irradiation therapy.32 Metal scattering could lead to three consequences: (1) a reduced dose of radiation to the tumor if it is situated behind implants, (2) a possible loss of osseointegration and implant failure due to higher radiation dose, and (3) an increased risk of osteoradionecrosis developing in the bone adjacent to the implant.33 In vitro studies employing a Monte Carlo approach found that the dose was 10% higher directly in front of an implant but almost 16% lower directly behind it relative to the dose in the plain phantom, due to differences in the densities of the two materials.3234 However, that study compared plain water and titanium implants, not bone and titanium implants, and the implant material and its surface coating can also influence the scattering. Implants containing gold exhibited a dose enhancement in the BIC area compared to pure titanium or Ti-6Al-4V alloy. One clinical study found three cases of tumor recurrence in patients who submitted to simultaneous implantation with ablative surgery; dose disturbance from radiation scatter was cited as one possible explanation.35 On the other hand, Stoll et al.36 reported dose increases of 12.5 - 16% at 0.45 mm from the metal specimen, but there was no influence on the life of the implant if the soft tissue was sufficiently thick. Pekmezci et al.37 also reported that current radiation therapy regimens may be performed without additional harm using linear accelerators. In other words, in a real treatment plan employing several beams from different directions, the overall effect will be spread over a larger volume and will be largely compensated for by the different beams. Until further data are available on the possible disadvantages of irradiation on titanium fixtures, avoiding the abutment connection or removal of all prostheses or frameworks before radiotherapy is recommended.38
CONCLUSION
Within the limits of this study, the timing of local irradiation critically influences the bone healing mechanism, which is related to osseointegration around implants. Irradiation resulted not only in retarded new bone formation around the implant during the early bone healing stage, but also that it partially affected retarded bone healing during the late bone healing stage. These findings are not in accordance with the results from previous studies which showed successful clinical results. However, implant placement before radiotherapy is still a valuable treatment modality considering bony site with poor healing capacity after irradiation. It would be recommended submerging the implant until tumor therapy (including radiotherapy) is complete, as well as using a longer healing period for nonirradiationa cases.






 XML Download
XML Download