

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Anomalies of tooth number, such as tooth agenesis or supernumerary teeth, result from developmental disturbances in the initiation and proliferation stages of tooth formation.1 Congenital tooth agenesis is defined as a state in which one or more teeth, excluding the third molars, are missing.2 Although various classification methods are available, tooth agenesis is usually classified according to the number of missing teeth; hypodontia, oligodontia, and anodontia refer to the states in which less than six teeth, more than six teeth, or all teeth, respectively, are missing.3 Among these, oligodontia has a particularly low prevalence (0.08-1.1%) and has been reported to be one of the symptoms of systemic diseases such as ectodermal dysplasia, Down syndrome, Nance-Horan syndrome, Rieger syndrome, and cleft lip and palate.4 Unlike syndromic oligodontia, mutations in PAX9, AXIN2, EDA, and MSX1 or environmental causes, such as drug-induced disturbances of the tooth germ and nutritional imbalances, are etiological factors in non-syndromic oligodontia.56
In most oligodontia patients, congenitally delayed tooth genesis and prolonged retention of primary teeth are observed, and unstable occlusion, such as traumatic occlusion and hypo-occlusion, occurs as a result of root resorption and ankylosis.7 Teeth in such cases are narrow compared with normal tooth dimensions, leading to dental anomalies such as microdontia or conical teeth. Excessive or insufficient restoration space can occur depending on the pattern and severity of tooth absence. Additionally, the absence of permanent tooth germ can result in severe atrophy of the alveolar ridge, which can pose problems in prosthodontic treatment involving implants.8 Patients with oligodontia often suffer from psychosocial impact in their childhood and adolescence due to their appearance and the inarticulate pronunciation that is caused by congenital tooth agenesis.9
Since any tooth on the dental arch can be missing, it is essential to evaluate the number and position of the missing teeth and residual teeth, and the state of the alveolar ridge during treatment planning. Malocclusion caused by retained deciduous teeth and congenital permanent tooth agenesis should be corrected, and space redistribution should be performed to make prosthetic restoration possible. Prosthetic restoration can be achieved by various methods, such as resin adhesion, fixed dental prosthesis (FDP), removable dental prosthesis, and implants; treatment options can be limited by the number and position of missing teeth and the state of the residual teeth and alveolar ridge. Given that conventional prosthetic treatment alone cannot achieve esthetic and functional rehabilitation, a multi-disciplinary team approach combining orthodontics, oral and maxillofacial surgery, and prosthodontics is indispensable. Early diagnosis using clinical as well as radiographic examination is essential and lifetime maintenance is also required. Comprehensive treatment goals should include restoration of stable occlusion and support for psychosocial adjustment by improving not only functionality, but also harmonious esthetics.
This case report writes about a patient diagnosed with non-syndromic oligodontia who received an FDP after orthodontic and implant treatment with a multi-disciplinary team approach.
CASE REPORT
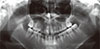
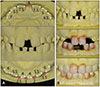
A 17-year-old patient visited our clinic for prosthetic restoration of her congenital tooth agenesis. She had no medical history of systemic diseases, but there was a familial history of partial oligodontia in her father and her sister. Extraoral examination revealed no abnormalities in the frontal and lateral facial profile, nor did lateral cephalometric radiographic examination reveal any skeletal anomalies. However, the panoramic radiograph revealed a total of 16 missing permanent teeth and external root resorption in some of the retained deciduous teeth (Fig. 1). A transcranial radiograph was taken to evaluate the temporomandibular joint. The joint function was normal and no clinical symptoms were observed, indicating that the condylar head was in a physiologically stable position. Intraoral examination revealed multiple deciduous teeth retained with spacing, an anterior open occlusal relationship (open bite), and an unesthetic smile due to diastema (Fig. 2). The retained deciduous teeth and permanent teeth resulted in mixed dentition. However, stable occlusion was present, with proper functioning without hypo-occlusion from ankylosis, despite the slight root resorption. Due to a poor tooth axis and loss of occlusal contacts, the anterior teeth could not properly guide mandibular protrusive movement. A diagnostic cast analysis showed a steep curve of Spee and an extruded mandibular left second molar, resulting in insufficient antagonist restoration space. Additionally, narrow maxillary central incisors led to a 5-mm interarch tooth size discrepancy (disproportion in the mesiodistal dimensions of teeth of opposing dental arches; Fig. 3A). Esthetic and functional problems, such as malocclusion, were local and limited to the anterior teeth.
These findings led to a diagnosis of non-syndromic oligodontia. Accordingly, the treatment goal was establishing anterior guidance and esthetics from solving the interarch tooth size discrepancy by restoring the missing teeth. With the involvement of an orthodontist, the initial treatment plan was decided to improve tooth axis and induce redistribution of the restoration space. A model of tooth arrangement, showing ideal tooth positions, was fabricated, and a diagnostic wax-up was performed on this model (Fig. 3B). After 11 months of the orthodontic treatment, teeth were re-aligned and diastema was closed (Fig. 4). After the orthodontic treatment and re-evaluation of the space and abutment, maxillary deciduous lateral incisors, canines, and mandibular deciduous central incisors were extracted because these teeth were risk factors for a poor prognosis. To minimize invasiveness, implants and FDPs were selected for treatment.
A face-bow transfer was performed to mount the diagnostic cast on a semi-adjustable articulator (KaVo PROTAR Evo 7, KaVo, Biberach, Germany), and the position of the incisal edge and gingival margin was designed, taking into account the shapes of the central incisors. The diagnostic cast was then reduced in accordance with the shape of the gingival margin, and a diagnostic wax-up was again performed (Fig. 5). Consequently, the initial interarch tooth size discrepancy of 5 mm was reduced to 2 mm. Irreversible hydrocolloid impression material (Aroma Fine Plus; GC Corp., Tokyo, Japan) was used to obtain an impression for fabricating a duplicate cast. On the duplicate cast, the lead embedded in the periapical radiographic film was cut to a 1-mm width and was positioned in the buccolingual cervical area of the diagnostic wax-up cast. A thermoplastic template (Duran 0.5 mm, Scheu Dental, Iserlohn, Germany) was used to fabricate a radiographic stent, and a cone beam computed tomography (CBCT) image was taken to evaluate the positional relationships between the bone, definitive prosthesis, and residual ridge. An additional bone graft was necessary at the maxillary deciduous lateral incisor and mandibular left deciduous canine areas due to the insufficient bone volume for implant installation (Fig. 6). In consideration of the patient's age and concerns about the surgical intervention required for the bone graft, the definitive treatment was changed to installing implants in the maxillary canine areas without bone graft, restoring the maxillary lateral incisors with a cantilever, and installing a mini-implant in the mandibular left canine area.
Prior to implant installation, mandibular teeth were prepared on the basis of the diagnostic wax pattern, and a provisional prosthesis was placed after extracting the deciduous anterior teeth. The position of the implant was chosen in accordance with the biological width and estimated gingival margin (Fig. 7). After extracting the deciduous canine without alveolar bone trauma, immediate implant installation was performed without invasion to the nasal floor, adjacent teeth, or nerve (Fig. 8). Tapered internal connection type implants (TSIV; Osstem, Busan, Korea) with a diameter of 4.0 mm and a length of 10 mm were installed in both maxillary canines, and a mini-implant (MS SA; Osstem) with a diameter of 3.0 mm and a length of 10 mm was installed in mandibular left canine. Immediate provisional restoration was placed after affirming the primary stability of the implant. All contact points during maximal intercuspation and lateral excursion were removed to minimize the stress exerted on the implant.
The emergence profile and the width-length ratio of teeth were improved with provisional restoration. Favorable shape and ratio of tooth to gingiva could be obtained using gradual adjustments. The narrow width of the central incisors was modified by widening the teeth using 0.5-mm resin application to the distal surfaces. The width of the lateral incisors was reduced and the gingival contour was gradually adjusted with a high-speed bur (Fig. 9). In order to set the lateral condylar path inclination and protrusive sagittal condylar path inclination of the articulator, protrusive and lateral occlusal relations (check bite) were recorded. Anterior guidance was established using provisional restorations. The adaptation of occlusion and esthetics was evaluated during the 6-week application.
The provisional restoration did not cause any noticeable discomfort. In the absence of mastication and pronunciation problems, a definitive prosthesis was fabricated. After taking a preliminary impression of the maxillary arch, a customized tray was fabricated. Pick-up impression coping was connected and autopolymerizing resin (Pattern resin LS, GC, Tokyo, Japan) was added to the gingival area to capture the soft tissue contour during impression taking procedures. Registration of the soft tissue around the mandibular central incisors was acquired using silicone bite registration material (Futar D, Kettenbach GmbH & Co. KG, Eschenburg, Germany) and a pick-up impression was taken (Fig. 10).
In attaching the master casts to the articulator with the cross-mounting technique, a customized anterior guidance table was fabricated to duplicate the anterior guidance of the provisional restoration. Full contour wax patterns were fabricated on the master casts, and titanium-based zirconia customized abutments (Myplant, Raphabio Co., Seoul, Korea) were fabricated via digital scanning. A zirconia coping was fabricated for the crown and internal adaptation was checked. Considering the inter-pupillary line and facial midline, the tooth axis was evaluated with the zirconia coping (Fig. 11). During an up-close examination while performing shade selection, a demineralized lesion was found on the buccal surfaces of the maxillary anterior teeth. In order to restore the shade of the teeth, resin infiltration was performed using unfilled resin (Icon, DMG, Hamburg, Germany) with an enamel-like refractive index. Then, a shade was selected and porcelain build-up was performed (Fig. 12). The definitive prosthesis was placed and adjusted to achieve mutually protected occlusion (Fig. 13).
In the follow-up examination after 18 months, oral hygiene was verified to be excellent, and there were no complaints in terms of occlusion, mastication, phonetics, esthetics, or the temporomandibular joint. The peri-implant marginal bone level was maintained without noticeable changes, and no abutment screw loosening or dislodgement of the cement-retained prosthesis was detected (Fig. 14).
DISCUSSION
Prosthodontic treatment alone is not sufficient to achieve ideal results in the treatment of congenital tooth agenesis in oligodontia patients; thus, a multi-disciplinary approach, including orthodontics or implants, is necessary.9 A definitive treatment plan for replacing the missing teeth should be decided after analyzing the state of the remaining teeth and the interarch relationship. Orthodontic treatment can improve the space redistribution of missing area, rearrangement of teeth, and correction of the tooth axis. Factors such as residual ridge configuration and the remaining bone amount can pose great challenges for prosthodontic treatment. In this report, the case was complicated due to migration of the adjacent teeth following multiple permanent teeth missing, limited restoration space, and abnormalities of the remaining teeth. Therefore, prosthetic restoration alone was considered insufficient for obtaining good esthetics and improving masticatory function, and thus the plan was decided to proceed to orthodontic treatment with prosthodontic treatment involving an implant.
It has been reported that missing permanent teeth make it difficult to provide good anchorage for orthodontic treatment.10 When 4-16 permanent teeth are missing, root resorption is likely to happen after orthodontic treatment.10 Another report has stated that deciduous canines and mandibular deciduous second molars could remain in the oral space longer than any other retained deciduous teeth. It has also reported that if a deciduous second molar still remained at the age of 20, good prognosis could be expected.11 However, if a deciduous molar was involved in hypoocclusion and was expected to hamper the growth of the alveolar bone through root ankylosis or resorption, it was necessary to extract it and replace it with an implant or FDP. Without the succeeding permanent teeth, the maxillary deciduous lateral incisors tend to be prematurely exfoliated and affect anterior esthetics; therefore, restoration after extraction should be considered.1112 After the diagnostic procedures in the case reported here, it was planned to extract the maxillary deciduous lateral incisors and canines and mandibular deciduous central incisors, because of their short root length and poor prognosis. During the orthodontic treatment, root resorption and pathologic tooth mobility of the mandibular left deciduous canine occurred, and thus an additional extraction was performed.
Congenital tooth agenesis is characterized by a narrower mesio-distal tooth width and a smaller dental arch size, and a smaller width of the remaining teeth is known to be related to a higher number of missing teeth.1314 Interarch tooth size discrepancy is defined as the difference in the sum of the mesio-distal dimensions of teeth of opposing dental arches; such discrepancy poses an esthetic problem and disturbs proper occlusal relations. In the anterior teeth, a discrepancy of about 2 mm is reported to be clinically problematic.15 In our case, the patient had a total of 16 missing permanent teeth; however, the esthetic and functional problems were local and limited to the anterior teeth. Additionally, the remaining teeth had were narrow and there was a discrepancy in the interarch tooth size. When comparing the patient's case with the ideal anterior Bolton ratio16 of the summed mesio-distal dimensions of the mandibular to those of the maxillary anterior teeth, the mandibular teeth width was found to exceed that of the normal range by about 5 mm. To resolve the interarch tooth size discrepancy and achieve an adequate arrangement of teeth for prosthetic restoration, the orthodontic treatment involved space evaluation through a diagnostic wax-up in a setup model.17 Orthodontic treatment resulted in tooth axis improvement and space redistribution, and the interarch tooth size discrepancy was reduced to 2 mm. In the definitive prosthesis, this discrepancy was further reduced to 1 mm by adjusting the provisional restoration.
In FDP, adequate crown width/length ratio and symmetry, as well as the gingival emergence profile, are essential for optimal esthetics. Rehabilitation of missing teeth was performed to improve the patient's smile using a diagnostic wax pattern after setting the position of the incisal edge and the gingival margin, taking into account the incisal edge exposure in the resting position and the curvature of the lower lip in a smile.
Implants were installed into the maxillary canine area about 2-mm palatally and 3-mm inferiorly to the gingival margin of the expected definitive prosthesis so that 1.8-2 mm of the buccal bone could be preserved.1819 The biological width was also considered. The provisional restoration was placed immediately after implant installation to sculpture the emergence profile. Excellent esthetics could be restored by gradually adjusting the gingival contour.
Maxillary and mandibular dental and skeletal growth leads to dramatic 3-dimensional changes in younger patients. Remodeling in the region of the implant installation site could cause several problems such as implants unsupported by bone or submerged within it, and loss of implants.20 However, implants placed during late puberty or early adulthood, like in our patient's case, have a good long-term prognosis.21
Dawson22 insisted that stable occlusion can be achieved by having stable occlusal stops in all teeth when the condyles are in a centric relation, avoiding interference of all posterior teeth, and having anterior guidance in harmony with the border movement of the envelope of function. The patient in the present report did not show any skeletal problems that might induce anomalies in the temporomandibular joint; it demonstrated normal function without any clinical symptoms, and the condyle was considered to be in a physiologically stable position.
With the missing permanent teeth and retained deciduous teeth, this patient developed an occlusion of mixed dentition that was functioning properly. However, the maxillary central incisors and mandibular lateral incisors were the only permanent teeth present on the anterior arch, exhibiting a poor tooth axis and loss of occlusal contacts. The anterior teeth could not guide mandibular movement, which resulted in occlusal interference of the posterior teeth. Therefore, a new anterior guidance had to be established using provisional restoration. The anterior guidance determined by the envelope of function was evaluated based on the patient's adaptation.22 Orthodontic treatment, implant installation, and gradual occlusal adjustment were used to establish stable, functionally harmonious anterior guidance (Fig. 14).
In this case, functional and esthetic occlusion was attained in a patient with non-syndromic oligodontia congenitally missing 16 permanent teeth through orthodontic treatment, followed by prosthetic restoration including implant. The treatment also brought about psychosocial adjustment in the adolescent patient. Although the patient demonstrate a stable function, lifetime maintenance is considered necessary due to some clinical factors specific to oligodontia.
CONCLUSION
This case report concerns a patient with non-syndromic oligodontia without any specific systemic disease. The patient was rehabilitated by means of space redistribution and prosthetic restoration involving an implant, through multi-disciplinary treatments. Optimal esthetics could be achieved by resolving the interarch tooth size discrepancy, gradually adjusting the gingival contour, and improving the crown width/length ratio. A new anterior guidance was established in accordance with function. In patients with oligodontia, lifetime maintenance care is essential for preservation of esthetics and function.












 XML Download
XML Download