

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Saliva has many functions that facilitates the swallowing of food, cleans the dentition, participates remineralization of tooth surfaces, serves as a digestive initiator and an ionic stimulator for taste.1,2 Saliva ensures a neutral pH, creates an oral environment and inhibits the harmful bacteria.3 It provides antibacterial, antiviral, and antifungal properties due to inherent agents (such as lysozyme, lactoferrin, peroxidase system and agglutinins) and other immune components that prevent adherence of microorganism to oral surface and effect microbial growth and metabolism.3,4
The decreased salivary flow rate has been associated with the xerostomia. The common causes of xerostomia are dehydration, medications, head and neck radiotherapy, diabetes mellitus and specific diseases.5 Xerostomia can diminish the quality of life, leading to inflammation of muccosal tissues, problems in dentures, and difficulties in eating, speaking, swallowing and taste function. Particularly in denture wearers, xerostomia seems to be a great problem to the clinicians, because xerostomia lead to the insufficiency in the wetting mechanism and denture retention, as well as change normal chemical composition of saliva and oral microbiota, and increase the risk for opportunistic infections, such as Candida albicans.6,7 Oral candidiasis is one of the most common oral infections seen in association with xerostomia and has been identified as an important causative agent for the pathogenesis of denture stomatitis.8
In the absence of saliva, administration of artificial saliva may be preferable to relief of dry mouth and suppression of infections such as candida. Various agents have been considered for patients with xerostomia that differ particularly in their base substance, chemical composition, or viscosity.9,10 Basically, these agents should have the same composition as natural saliva, nevertheless most of these artificial salivas have only compounds to enhance lubrication and moistening.11 However, saliva contains antimicrobial proteins with enzymatic activity such as lysozyme, lactoperoxidase and lactoferrin.12 Since the 1990s their antimicrobial activity in the oral cavity has been shown, these enzymes have been proposed for use in xerostomia patients with the aim of preventing related disease.7,8 However, up to date, the knowledge on the antifungal and antiadhesive activity of commercial artificial saliva substitutes is limited.8
With regard to this aspect, the aim of this in-vitro study was to compare the effect of two artificial salivas on the initial adhesion of Candida albicans. It was hypothesized that adhesion of Candida albicans to acrylic surface will be lower in the Biotene Oral Balance gel containing lysozyme, lactoferrin.
MATERIALS AND METHODS
The wax pattern of the specimens (diameter 10 mm, thickness 2 mm) were prepared from stainless steel mould and were invested in the dental flasks directly in dental stone for water-bath polymerization. After the gypsum had set, the flasks were boiled to soften and eliminate the wax, and stone surface were painted with a separating medium. The acrylic resin (Acron Duo, Surton, Swindon, England) was prepared according to the manufacturer instructions and then was packed into the moulds. After completion of polymerization, all flasks were allowed to cool for at least 3 h. Then the acrylic resin disks were trimmed using metal bur. Each acrylic resin specimen was abraded manually with emery paper (grit 400) in a figure-of-eight motion. A total of 45 acrylic specimens were prepared for three groups; control and two salivas (n=15). Acrylic resin specimens were stored in sterile distilled water to remove any residual monomer for one week at 37℃. To check surface roughness of specimens, ten of specimens were randomly selected and surface roughness was measured using profilometer (Surtronic 10, Taylor Hobson Ltd, Leicester, England). Three readings were performed for each specimen (one in central, two at the margins) and the mean of three readings was recorded as the Ra value of specimen. Surface roughness values ranged between 0.08 µm and 0.2 µm was accepted as references.
The next, acrylic specimens were sterilized in autoclave for 18 min at 1.2 bar, 121℃ (Charisma vacuum TD, Mediline Italia, Cavriago, Italy). Before Candida albicans contamination, specimens stored in distilled water at 37℃ for 24 hours.
The strain C. albicans (ATCC 90028) was inserted in a horizontal shaker (Barnstead International, Dubuque, IA, USA) and was incubated in Sabouraud dextrose broth (Sigma Aldrich, Inc., St. Louis, MO, USA) supplemented with 500 mmol/lt sucrose for 24 hours at 37℃. The culture was then centrifuged (Nüve Nf 1215, Ankara, Turkey) at 1700×g for 10 min and the resultant cell pellets were washed twice with 0.15 mol/lt phosphate-buffered saline (PBS) solution at pH 7.3. Cells were resuspended in PBS and a standardization of the yeast suspension to 1×107 yeast/mL was obtained by spectrophotometer (Shimadzu UV-1201, Shimadzu Precision Instruments, Torrance, CA, USA).
Two commercial artificial salivas were used which are Saliva Orthana and Biotene Oral Balance gel. The manufacturers and components of these materials were listed in Table 1. The sterile distilled water was used as control group. All of the specimens were randomly distributed three groups containing 15 acrylic resin discs in each experimental group and specimens were stored in the artificial salivas or in the sterile distilled water for 60 minutes at 37℃. Then, specimens were removed from artificial saliva substitutes and washed with sterile distilled water for 10 seconds and incubated for 24 hours at 37℃.
The acrylic resin specimens were placed to yeast suspensions at 37℃ for 3 hours in horizontal mixer. The specimens were then washed in sterile distilled water to remove non-adherent cells and left to dry in room temperature. Following the washing procedure, the specimens were inserted on glass slides and gram stained 30 seconds and the adherent yeast cells were quantified using ×40 magnifications under a light microscope. Adherent yeast cells were enumerated in 10 different fields of each specimen and the mean value of ten fields were recorded as adherent yeast cells of each specimen that were then scored according to Table 2.
Statistical analysis was performed by using the SPSS 16.0 software package (SPSS, Chicago, IL, USA). The comparison of groups was analysed with the Kruskal-Wallis test given the small specimen sizes and lack of normality in the data. Then post-hoc comparison was performed using Mann-Whitney U test between experimental groups. Differences was considered statistically significant at P <.05.
RESULTS
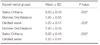
The adhesion scores of Candida albicans in two artificial salivas and distilled water are shown in Table 3. Results of Kruskal Wallis analysis indicated statistically significant difference in adhesion of Candida albicans among experimental groups (P=.000). Table 4 shows the mean values and standard deviations of adhesion scores and the results of Mann Whitney U post-hoc test analysis (P<.05). Saliva Orthana had higher adhesion scores than the Biotene Oral Balance gel and distilled water.
DISCUSSION
Saliva plays an important role in the preservation and the maintenance of oral health and function11 that provide remineralization of dentin and enamel and help maintain a healthy oral flora including lactoferrin, lysozime, lactorperoxidase and immunoglobulin.5,13 Accordingly, decrease in salivary flow rate contributes to an increased risk of infections such as Candida albicans.6,7
Candida albicans is the most important and predominant oral fungal pathogen.14 In colonization and the pathology of the disease, adherence of Candida albicans to acrylic resin surfaces is important and primary step,15 therefore the inhibition of adhesion of Candida albicans to oral surfaces is thought to be an important step in preventing oral candidiasis and most of the studies focused on the inhibition of adhesion of Candida albicans.8,16,17,18,19 It has been stated that the adhesion of Candida albicans to acrylic surfaces depends on the physical properties of the material surface such as porosity, surface free energy, hydrophobicity and roughness.14 However, when the denture is inserted into the oral cavity its surface is rapidly covered by a fine film of saliva.16 Saliva converges the hydrophobicity values of all oral surfaces, 20 diminishes the effect of the surface roughness of the materials, and alters the surface free energy.17 In substance, the salivary pellicle reduces the difference in candidal adhesion between the materials. Therefore, components of saliva become important. It has been stated that the adhesion of Candida albicans to oral surfaces is modulated by different salivary components, including mucins and other salivary proteins and secretory IgA (sIgA).22 The effect of these components on the adhesion of Candida albicans to oral surfaces may be very different, while some of them can increase adhesion, others can lead to inhibition.21
For management of xerostomia several commercial artificial saliva products with different components have been used. The present study compared the influence of two types of artificial salivas which are Biotene Oral Balance gel and Saliva Orthana. Biotene Oral Balance gel contains lysozyme, lactoferrin and peroxidase system that their antifungal properties have been reported.23,24 In addition to these enzymes, to make lactoperoxidase enzyme antimicrobial, its substrates, thiocyanate (SCN±) and hydrogen peroxide (H2O2), are also needed.24,25 Thiocynate were included in Biotene Oral Balance gel, however H2O2 is generated by glucose oxidase. Glucose oxidase is added to this preparation to complete the peroxidase system that generate H2O2 by catalyzing glucose in situ in the mouth, which serves as a substrate for lactoperoxidase.24 One of the other advantages of peroxidase is that administered lactoperoxidaseenzyme rapidly consumes intraorally generated H2O2 (by aerobic bacteria) whose accumulation in the mouth could be detrimental to oral mucosal cells.24 Other substance Saliva Orthana mainly include mucin that has been reported to absorb Candida albicans in significantly greater quantities than other proteins such as lysozyme and fibrinojen.26 Other components of Saliva Orthana are xylitol and fluoride that are mainly essential in caries prevention and it has been stated that fluoride has weaker antifungal activity and might be used as a support therapy for oral candidiasis.27
In the present study, Biotene Oral Balance gel showed a statistically significant lower adherence when compared to that of Saliva Orthana. It was probably due to the included components of products such as lysozyme, lactoferrin and lactoperoxidase that their antimicrobial actions in oral cavity have been shown in many studies..11 Hahnel et al.8 investigated influence of the commercial artificial salivas on initial adhesion of Candida albicans and stated that artificial saliva containing lysozyme, lactoferrin may be useful for possibly inhibiting Candida albicans adhesion to oral interfaces. They suggested that artificial saliva may be an initial point for treatment method influencing the oral microbial flora including Candida albicans.8 On the other hand, Sugiura et al.28 investigated the antimicrobial efficacy of artificial saliva containing lactoperoxidase, lysozyme, and lactoferrin (Biotene Oral Balance gel) against several microorganisms and found of no transparent zone for Candida albicans, but growth was inhibited in the area where Biotene Oral Balance gel was applied. On contrary of present results, Güneri et al.12 evaluated antimicrobial activity with diameter of the inhibition zones and found no antifungal effect of the Biotene Oral Balance gel saliva substitutes. The different results of these studies may depend on the use of different antimicrobial methods. And recently, instead of the initial adhesion of Candida albicans, the effect of artificial salivas in biofilm formation of Candida albicans has been evaluated by Silva et al.7 They found that Biotene Oral Balance gel had higher biofilm formation compared to the that of artificial saliva which is composed of carboxymethylcellulose.7
In the present study, both of the artificial salivas have shown higher Candida albicans adhesion than control group (distilled water). These results support that components of saliva may increase Candida albicans adhesion to acrylic resin denture.18,21,22 In agreement with present results, Henriques et al.18 stated that in the presence of artificial saliva number of adhered Candida albicans was greater than distilled water. The authors explained this result with high ionic strength of artificial saliva which has a direct influence of on electrostatic interactions established in the adhesion events.
The main limitation of present study was in-vitro nature of the present investigations with small number of specimens. In addition, only two artificial saliva substances were tested and only Candida albicans was evaluated. Other candida species and saliva substitutes may change the obtained results. Further both in-vivo and in-vitro studies with larger specimen size are needed to elucidate efficiency of artificial saliva substitutes on adhesion of Candida albicans.
CONCLUSION
In the present study, Biotene Oral Balance gel containing lysozyme, lactoferrin and lactoperoxidase resulted lower Candida adherence compared with Saliva Orthana. Inhibition of adhesion of Candida albicans to oral surface thought to be an important strategy in preventing oral candidiasis, therefore use of artificial salivas including these enzymes in comparison to conventional artificial saliva substitutes may be an appropriate treatment method to prevent adhesion of Candida albicans and related infections in patients with xerostomia.



 XML Download
XML Download