

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Nowadays changing the position of inserted implants is done in individual clinical experiments. In many cases the integrated implants are not in an appropriate position and can cause pressure to the dental nerves, maxillary sinus membrane damage or many difficulties in prosthetic procedure due to incorrect implant direction. On the other hand the implant may rotate during the abutment screw tightening or prosthetic treatment in immediate, early or delayed loading.1 During these procedures a sheer force is transmitted to implant-bone interface. This strength obviously has a detrimental effect on the bone next to the implant and could lead to disintegration.2,3
Rotation of an implant after eight weeks of healing, based on contractual implant success benchmark, could be a sign of failure and in this situation implant removal would be planned even in the absence of the other established indicators of non-osteointegration.4,5,6,7,8 In other words loose implants are considered as failure and are prescribed to be removed.1 But several studies have shown that loose implant can result from the absence of bone-implant contacts,1 and is not considered as the failed implant.1,9,10,11 There is a difference between rotational mobility and buccolingual mobility.2
According to observations from clinicians, despite the possibility of non integration implicated by the rotation,4 it seems acceptable if the implant is allowed to heal for an additional period of time, integration of an implant can be re-established.1,12 Considering the resistance to 20 Ncm reverse torque is a parameter for osseointegration and a measure of functional stability,13 so clinicians have to decide how long they should wait for re-integration of the implant or when they should remove it from the mouth.2 However, there are very limited data supporting their decision at present.2 There is no basic and fulfilling study in this field therefore more research due to the increasing use of implant in the world and also the interest in early and immediate loading of implants is needed.2,4
This investigation is designed to find the answer to two questions: First, the best time and the success of counter torquing or transposition of inserted implants, second: whether it is possible, for any given reason, to transport implants in the bone once they are integrated.
MATERIALs AND METHODS
Five male adult dogs weighting 25-30 kg were used in this investigation. The protocol of this study was approved by the Ethics Committee of Shahid Beheshti University School of Dentistry, Tehran, Iran, and the National Animal Care Society, Tehran, Iran. A period of 10 days was considered to standardize the diet and environmental conditions of the dogs.14
All the procedures were done by one clinician. An overall number of thirty implants (Implantium, Republic of Korea, 3.80 mm × 10 mm) were used in this study, that is, three in each dog's tibia making it six for each individual dog. The consensus on dividing implants into six groups was made: 1) one week control (1WC), 2) eight week control (8WC), 3) one week counter torque (1WCT), 4) one week transposition (1WT), 5) eight week counter torque (8WCT); and 6) eight week transposition (8WT). All dogs received the whole six implant groups.
For 12 hours the dogs were in full non-diet regime before operation with no water for four hours. An intramuscular (IM) injection of ketamine 10%, (10 mg/kg) (Rotexmedica co, GmbH, Germany) and Xylazine 2%, (1 mg/kg) (Behyar Saman Pharmaceutical Co, Tehran, Iran), was used to sedate the animals prior to operation. The IV injection Sodium thiopental 5% (Behestan Darou Co, Tehran, Iran) with average dose (10 mg) was used for general anesthesia. The tibia was rinsed thoroughly with Saline (Shahid Ghazi Pharmaceutical Co, Tabriz, Iran) and Povidine-iodine (Tolid Darou Co, Tehran, Iran). Following operation, animals were taken care of according to the protocol of Tehran Veterinary School, Tehran, Iran, with a special diet and supporting medicament. Prophylactic IM 6.3.3 Penicillin (Jaber Ebne Hayan Laboratories, Tehran, Iran), Dexamethasone 2 cc (Darou Pakhsh, Tehran, Iran), B complex 2 cc (Exire Pharmaceutical Co, Tehran, Iran), Mefenamic capsule 250 mg (Razak Laboratories, Tehran, Iran) per 12 hours and Tramadol tablet 100 mg (Razak Laboratories, Tehran, Iran) per 12 hours was administered daily. The presences of edema or inflammation in the area of sutures were inspected. The sutures were removed on the seventh or twelfth day following surgery.
The sterile conditions were maintained throughout the operation.
Week 0: For surgical procedures, the animals were anaesthetized. The surgical implantation was performed through a crestal incision4 and the tibia metaphyses were exposed by full thickness flap and with the ample reflection of the periosteal flap.4 One implant was inserted in the proximal part of each tibia (two implants in each dog) during vigorous irrigation with sterile saline.1 The implants were inserted 1 mm subcrestal in bone (Fig. 1).
Week 1: After one week, in second session, all animals were anaesthetized for the second time, as described above.1 Randomly, one implant in one tibia of each dog was counter torqued by applying a reverse force with a ratchet and the implant in another tibia was transposed. Also, three new implants were inserted in each dog so that the two implants in two different tibiae in each dog were considered as the eight-week group and another one was considered as the first control group (Fig. 1).
Week 9: After eight weeks, during the third session, the one week group implants and first control group implants were counter torqued using Mark-10 universal torque series sensor STW and the force values were read using a Mark-10 Force/torque Indicator Model BGI (JLW Instruments, Chicago, IL, USA).4 The torque sensor was fitted with a special extension attached to the implant mount for access,4 Once connected, the torque indicator system was placed in peak-force ready mode,4 and the increasing counter torque was applied until the detachment from bone was observed,4 then peak value was measured,4 and the display on the indicator was recorded.4 The implant was then pro-rotated back in to its original position. Afterwards, one implant which was not manipulated was counter torqued and another one was transposed in each dog (Fig. 2A, Fig. 2B and Fig. 2C). Thus, one new implant (in the tibia that had only two implant) was inserted in each dog that would be assumed as the second control group (Fig. 1).
Week 17: After another eight weeks, during the fourth session, the eight-week group and second control group implants were counter torqued to lose by applying STW and BGI which recorded the peak force required to detach the implant. The implants were then returned to their pre counter torque position (Fig. 1, Fig. 2D and Fig. 2E).
The data were analyzed with One-Sample Kolmogorov Smirnov and Leven. Thus, the groups were compared from the view of integration (Ncm) with Complete Randomized Block ANOVA. Statistical differences are indicated if P <.05.4
RESULTS
There were 30 implants that were inserted in 5 dog tibiae. They were assigned to six groups for study: 1) first control; 2) second control; 3) 1 WCT; 4) 1WT; 5) 8 WCT; and 6) 8 WT. All the manipulated and non-manipulated implants were osseointegrated. Two of the implants in dog #1 of the 8 WCT and 8 WT groups could not be liberated because the hexes of the implants were stripped. Therefore they were excluded and the second control in dog #1 was excluded accordingly. During the third and fourth sessions of surgery a very thick bone was formed above the fixtures, they were carefully removed with trephine drills so that the implants were not injured.
The data of total 6 groups confirmed the normality with using One-Sample Kolmogorov with minimum eventuality of 0.796. Data variance equality was studied and assigned to three groups related to 1 week (first control - 1 WCT - 1 WT) with eventually 0.288 and in three groups related to eight week (second control - 8 WCT - 8 WT).
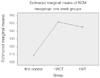
For comparing the quantity of osseointegration (Ncm), Completed Randomized Block ANOVA in three groups (first control - 1 WCT - 1 WT) was used. No statistically significant difference between the research groups (P=.052) was shown. However the mean quantity of osseointegration revealed differences in the three groups (first control - 1 WCT - 1 WT) but they were not significant (Table 1). The mean is described in Fig. 3.
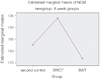
In order to compare the quantity of osseointegration (Ncm), Completed Randomized Block ANOVA in three groups (second control - 8 WCT - 8 WT) was used. No statistically significant difference between the study groups (P=.121) was shown. But the mean quantity of osseointegration displayed differences in the three groups (second control - 8 WCT - 8 WT) but they were not significant (Table 2). The mean is described in Fig. 4.
In this manner, No significant difference was discovered between the two study groups (first control - 1 WCT) with P=.90, two research groups (first control - 1 WT) with P=.116, two study groups (second control - 8 WCT) with P=.145, two research groups (second control - 8 WT) with P=.536, two research groups (1 WCT - 8 WCT) with P=.234, two study groups (1 WT - 8 WT) with P=.592.
DISCUSSION
The increased demand for early and immediate loading treatment plan in patients with implant supported dentures has led the clinicians to unscrew the implant's cover screw earlier. Regrettably, these installed implants may not have adequate primary stability. Therefore, they might rotate in the bone socket. This procedure is also likely to occur during abutment screw tightening. However, this eventuality could be expected because of not having adequate time for osseointegration.1,2,4
Bone healing around the implant depends on different factors. The stem cells which migrate there are only transformed into fibroblast as a result of micro movements then consequently fibrointegration occurs. So a parameter of assessing the attainment of osseointegration is a resistance to minimal 20 Ncm reverse torque for preventing micromovement.4,12 Many clinicians have tacitly accepted the counter torque test as a clinical indicator of successful integration.4,12,15
Currently, researches emphasize the formation of a strong bed for implant by a 'second callus'. Establishing and superimposing of this callus to the primary healing response will produce a stronger implant bed.4 Another implication could be when implants were not inserted in an appropriate place or in close proximity to anatomic area such as maxillary sinus, inferior alveolar nerve and mental foramen. In these cases which force the implants to exit, the evaluation of the effect of utilizing counter torque is required.4,16
The present study is solely aimed at the clinical assessment of the resistance of implant following counter torque test in two intervals of one week and eight weeks. Definitely, this research should be confirmed by further histopathologic evaluation. The results of this study are supported by the findings in previous reports. In our study, reintegration is possible after counter torque test is carried-out on integrated implants. This outcome was achieved after eight weeks as healing time in eight-week rotation groups. The results of the present study also confirm the findings of Moriya et al.2 while the counter torque is closer to implantation time, the result is more preferable and even higher than the control group. However, this was not observed in Lucente et al.4 study. The samples of the Lucente's research were 11 humans therefore the number of the implants was statistically lower than this study.
The present study showed that implant reintegration is possible after counter torque test (physical dislocation of the implant from the healing bone) in integrated implant.4 The result refers to the eight-week rotation groups. This is in accordance with findings of Ivanoff et al.1 and Lucente et al. In the animal study of Morberg and Albrektsson,17 who used rotational strain to the implant to break osseointegration, subsequent integration was achieved.2 Several studies have reported good prognosis of rotated implants finally functioned without any clinical difference from non-rotated implants.2,18,19,20
Transposition of the implant have been reported only in rare situations when the implant has been transposed with its surrounding bone to correct the implant position.21 However in the present study, for the first time, implant transposition has been carried out without surrounded bone and, with/without detachment, the implant was separated from the adjacent bone and installed in the other cavity. A number of them were removed one week and the others eight weeks after the implantation. They were reimplanted in another site without any interruption.
The evaluation of the implants after eight weeks healing process revealed that the osseointegration has occurred. The mean value of the 1WT group (145/20 Ncm) has been increased in comparison with the control group (109/40 Ncm). On the other hand, the mean value of the 8 WT group (152 Ncm) has decreased in comparison with the control group (182/60). This is considered a suitable osseointegration while the implant surface is covered with some osseous particles and its uncontaminated transposition from one cavity to another will cause osseointegration.
Following the implantation, the clot is formed around the implant. This clot will then be organized after two days and the fibroendothelial cells and angiogenesis are observed. Also, because of different growth factors released, especially TGF (Transforming growth factor), there will be a proper condition for migrating and differentiating of cells that make up osseous matrix. An important factor in the first week is the high number of stem cells and osseous callus that are highly elastic. Also, due to the presence of stem cells, osteoid will be secreted and the calcification will take place. Therefore after the counter torque or transposition, the osseointegration will be achieved, proceeding the repair/healing phase. These values are higher than the control group. The important point in this time is that the implant surface is covered with GF (Growth Factor), stem cells, young connective tissue and primary osteoid. After eight weeks, the woven bone is formed at the site, the elastic callus is not present at this time, and if the counter torque or transposition is applied, due to the secondary pressure site, the resorption is also probable.22 Even though following bone detachment some bone particles remain on the implant surface and cause new sites of early junctions.
Based on the Frost theory of the Regional acceleratory phenomenon (RAP),1,23,24,25 which is one aspect of healing after operation, a noxious stimulus speeds up bone modeling and remodeling.1 Therefore one can hypothesize that bone detachment from the implant as a result of counter torque or transposition leads to the activation of the cytokines (e.g., TGFβ1, aFβF, bFβF and BMP2,7), which is the same mechanism as in any other traumatic event in the bone.4,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41 According to the mechanism of the action described by Davies,4,16 it seems that the areas that did not have adherent bone were likely to be saturated with blood released from disrupted local vessels after the counter torque or transposition.4 In other words the reintegration success in these implants may be a function of the cellular processes in which the surfaces attach and secure the blood clot,4 anchoring fibrin that provides a pathway for the osteoblasts to migrate to the surface of the implant and initiate de novo bone formation.4 Therefore, at final evaluation, the counter torque force also had to overcome the resistance provided by newly formed interfacial bone.4,16,42
This research showed that if the implant was counter torqued or transposed after one or eight weeks following implantation, osseointegration was achieved after the healing period.
CONCLUSION
The conclusions of this study are those that follow:
After the counter torque process, one week or eight weeks following the implantation, osseointegration was achieved. After transposing the implant, one week or eight weeks following the implantation, osseointegration was achieved. Comparing the one week and eight week intervals, the one week would result in a stronger osseointegration, when comparing to the values with the control group. Comparing the one week and eight week intervals, the implant transposing after one week is suggested due to its better results.




 XML Download
XML Download