

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Bar-retained implant overdentures (IODs) are a common treatment option in implant prosthodontics, and the implants that support the prosthetic restorations exhibit high survival rates.123 It has been discussed controversially if the number of implants or a placing of extensions on bars influence the clinical outcome of IODs.45678 However, the data on the prevalence of biological complications remains limited.910 It has been proven that the bone resorption for IODs on prefabricated bars is lower in comparison with IODs on cast bars.11 In contrast, a systematic review demonstrated similar bone loss around implants supporting IODs with different attachment designs.12 This retrospective study examined the survival and success rates as well as the prevalence of peri-implantitis of IODs retained by 3 different bar designs.
MATERIALS AND METHODS
This study is based on patient files from the departments of Maxillofacial Surgery and Prosthodontics of the University Medical Center Goettingen. It was approved by the local ethics committee (approval no. 1/9/09). Twenty-seven patients (16 female, 11 male) were treated between 1991 and 2006 with IODs (n=36) that were retained by 3 different bar designs (group A=prefabricated round bars without extensions, resilient anchorage, n=7; group B=one-piece anterior milled bars with distal extensions, rigid anchorage, n=20; and group C=two bilaterally placed milled bars, with distal extensions, rigid anchorage, n=9) on 4 to 6 implants (2 - 3 per side) (n=161, mean: 4.5 per jaw) in the mandible (n=24) and/or in the maxilla (n=12).
Inclusion criteria for the study were in compliance with annual recall intervals, a post-operative (baseline) panoramic radiograph, and at least one follow-up panoramic radiograph after a minimum observational period of 5 years (mean: 7.3 ± 3.6 years; range: 5-19 years). Furthermore, the complete documentation of all implant- and prosthesisrelated technical complications was mandatory for inclusion in the study. All radiographs were digitally analyzed (Adobe Photoshop CS4, San Jose, CA, USA). Calibration was performed by referencing the documented implant length. The marginal bone levels were calculated on the basis of the radiographic linear distance from the implant shoulder to the first bone-to-implant contact (Fig. 1). Radiographic bone loss during the functional period was calculated by subtracting the linear distance from the implant shoulder to the marginal bone level at baseline from the distance from the implant shoulder to the marginal bone level at the last available radiograph.
Bone loss ≥3.5 mm was defined as "peri-implantitis".91013 Furthermore, all prosthodontic maintenance was recorded for the survival and success analysis according to Kaplan-Meier. Technical complication rates for each type of restoration were analyzed and compared via one-way ANOVA and the Chi-squared test (Software R version 2.8, www.r-project.org). A type one error of <0.05 was accepted as statistical significance.
RESULTS
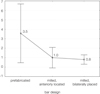
Two implants (one in the maxilla after 7 years and one in the mandible after 6 years) had to be removed (7-year survival rate: 97.7%). All IODs remained in function (7-year survival rate: 100%). In total, 70 of the technical complications (attachment-related: 49%, denture-related: 51%) required clinical intervention to maintain the function of the IODs (overall technical complication rate: 0.37 treatments per patient per year (T/P/Y)), (Table 1). Technical complications occurred more frequently in group A (mean: 3.5 during observational time) than in the other two groups (B: 0.8: C: 1.0). However, this difference was not statistically significant (P=0.58, Fig. 2). The success rates (Kaplan-Meier) which represent the share of IODs that were functional without any clinical intervention are presented in Fig. 3. Peri-implantitis was diagnosed in 20 implants (12.4%), in 12 IODs (3 in the maxilla, 9 in the mandible) (A: 2; B: 9; C: 1) in 10 of 27 patients (37%). Six of the 10 smokers (60%) that participated in the study, and 4 of the 17 non-smokers (23.5%) were diagnosed with peri-implantitis (Fig. 4).
DISCUSSION
The implant (97.7%) and prosthetic (100%) survival rates are similar to the findings reported by other studies.123 In literature, the requirements for prosthetic maintenance of IODs vary between 0.25 and 4.03 (T/P/Y).12310 The overall technical complication rate of 0.37 (T/P/Y) that was calculated in the present study is at the lower end of this range, it is similar to other studies that reported technical complications of bar-retained IODs.12 In the present study, IODs that were retained by milled bars exhibited rather lower but statistically insignificant rates of mechanical complications in comparison with IODs retained by prefabricated round bars. Nevertheless, this is similar to previous studies that reported lower technical complication rates for milled bars than that of prefabricated round bars.12 Krennmair et al.6 (2012) demonstrated high implant success rates and limited prosthodontic maintenance for rigid anchoring with milled bars or telescopic attachments. In this study, bar-related complications predominantly appeared for prefabricated round bars, whereas IODs retained by milled bars showed more denture-related complications. Bressan et al.14 (2012) also demonstrated mainly bar-related complications for IODs retained by round bars supported by two implants. Alternatively, Heschl et al.15 (2013) documented only limited complication rates for round bars supported by 4 implants with distal extensions. Other authors controversially discussed whether the number of implants and/or the use of extensions have an impact on the complication rates of IODs. Ueda et al.8 (2011) and Meijer et al.7 (2009) found no differences between IODs supported by 2 or 4 implants. However, Krennmair et al. (2007 & 2012) demonstrated prevention of non-axial overloading, posterior bone resorption or denture rotation for bar-structures rigidly retained by 4 implants.567 Moreover, up to now, the relevance of extensions regarding the complication rates of IODs seems indistinct. Placing cantilevers on bars was rated useful to offer adequate occlusal posterior support.4 However, Krennmaier et al.5 (2007) showed that distal extensions included in their bars affected neither the degree of distal bone loss nor the implant survival rate. Nevertheless, in the present study round bars on 2 implants without extensions offered higher complication rates than milled bars on 4 implants including distal extensions.
In the present study, 12.4% of the implants in 37% of the patients exhibited radiographic symptoms of peri-implantitis. Studies using the same diagnostic criteria have reported implant-based peri-implantitis rates between 10.1-11.7%, and patient-based peri-implantitis rates of 9.2-10.0% for mean observational periods of 5.6-7 years.910 The bar design might explain the comparatively high peri-implantitis rates in the present study. It may lead to a reduced accessibility for oral hygiene procedures at home.10 IODs retained by milled bars exhibited significantly higher plaque index values than IODs retained by telescopic crowns.6 In the present study, especially massive one-piece milled bars in the mandible showed radiological symptoms of peri-implantitis (9 out of 20, however, the rates were not statistically significant). Abd El-Dayem et al.11 (2009) demonstrated less bone resorption for IODs supported by round bars compared to custom-made bars. In the present study, smoking patients exhibited a higher prevalence of peri-implantitis than non-smoking patients (60% vs. 23.5%), thus supporting data from previous studies suggesting that a smoking habit is a significant risk factor for the development of peri-implant diseases.9
CONCLUSION
Within the limitations of this study, we concluded that barretained IODs are an adequate treatment option for edentulous jaws. These restorations may exhibit high implant and prosthesis survival rates (>97%) and a limited incidence of technical complications after a mean observational period of >7 years. Nevertheless, peri-implantitis was identified as a frequent and serious biological complication for this type of reconstruction.




 XML Download
XML Download