

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Tooth loss is a major problem worldwide, one with adverse oral, systemic, and mental health effects. Edentulous participants experience such difficulties as problems chewing food,1 weakened facial musculature, degradation of the supporting alveolar structures, reduced bite-force and chewing efficiency,2 gastrointestinal disorders,3 and difficulties with socialising or forming close relationships.4 Rehabilitation with prosthesis can alleviate these adverse effects to some degree and provide a sense of normalcy, allowing the patient to interact with others.5
Removable prostheses have been used as one method to make up for missing teeth for a long time.6 However, exaggerated gag reflex may lead to problems during the production and wearing of removable complete and partial prosthesis. The gag reflex can be triggered by bad prior dental experiences,7 dental anxiety,8 the thought of something being placed in the mouth,9 excess saliva accumulation when the patient refuses to swallow for fear that the denture will dislodge,10 the touch of the mirror or impression tray on trigger points, or even the sight of these materials.11
The patient part of the short form of the Gagging Problem Assessment Questionnaire (GPA-pa SF) is a shorter version of a longer questionnaire introduced by van Linden van den Heuvel et al.12 and gives information about patient's self-reported gagging severity. The GPA-pa SF is a Likert type scale and includes nine questions about the patient's own perceptions with respect to any gag reflex activity that may occur when procedures involving dental hygiene, examination, or impression taking are being carried out. Conditions which are not suitable for the individuals are rated as not applicable and these questions are not included in the calculation of the total score.12
To our knowledge, no study to date has evaluated factors including, gender, education level, prosthesis type and patients' tolerance to removable prosthesis according to the GPA-pa SF. Therefore, the aim of this study was to assess removable prosthetic restoration tolerance according to the patient part of the short form of the GPA-pa SF and influence of gender, education level and prosthesis type on the GPA-pa SF scores over 2 months after prosthesis insertion.
MATERIALS AND METHODS
This study was conducted at Gazi University's School of Dentistry in Ankara, Turkey. The university serves a large patient community, including civil servants, public sector employees and their dependants (housewives or selfemployed). It also has the necessary staff and equipment for performing dental procedures under sedation or general anaesthesia. The study was approved by Ankara University Local Ethics Committee (No. 39-5). All participants gave their informed consent in writing before participating in the study.
A medical history was obtained, and a routine dental examination procedure was performed. A total of 130 participants who did not have any chronic or acute disease, and who were not taking medications to treat any chronic or acute systemic disease or dental pathology were started to participate in the study. Participants were excluded if they were pregnant or had any mental or physical disability or psychological disorder. Participants were asked to complete a standard form, containing questions about age, gender, education level, and dental attendance. Participants were administered the Turkish version of the GPA-pa SF, which has been shown to be a valid and reliable translation of the English form.13 The type of prosthetic restoration was recorded by a prosthodontist who did not ask the questions on the standard form (Table 1). The GPA-pa SF was completed before the prosthetic restoration (T0), and 1 day (T1), 2 days (T2), 15 days (T3), 1 month (T4), and 2 months (T5) after denture insertion. The questionnaire was read aloud to participants, and they were asked to estimate their sensitivity in terms of gagging for the applicable situations. Situations which were not applicable for patients was marked as not applicable on the questionnaire (for example; "brushing your teeth" was marked as not applicable for edentulous patients).
Preliminary impressions were made with alginate (Cavex CA37; Cavex Holland BV, Haarlem, the Netherlands) by using a stock tray (Inci Dental Tıbbi Malzeme San. ve Tic. Ltd., Istanbul, Turkey). For 15 participants (14 females), impressions were made with the aid of a topical anaesthetic solution, (Vemcaine, 10% lidocaine; Nobel Farma Ilaç San. ve Tic. A.Ş. Sancaklar, Düzce) disinfected with Deconex (Borer Chemie, Switzerland). After impressions were sent to the dental laboratory, diagnostic casts were obtained. Custom trays were fabricated on the upper and lower jaws with autopolymerizing acrylic resin (Vertex™, Zeist, Netherlands) by a dental technician.
For complete dentures, border molding was done with an impression compound material (Kerr, Italy), and final impressions of the upper and lower edentulous arches were made with zinc oxide eugenol impression paste (Cavex, Holland). For removable partial dentures, final impressions of the arches were made with alginate. Impressions were disinfected and poured with type III dental stone (Denston 3, Ata Yapı Ürünleri San. Tic. Ltd., Şti. Istanbul, Turkey) to obtain the master casts. Record bases were fabricated from autopolmerizing acrylic resin (Vertex™, Zeist, Netherlands) on the master casts for complete dentures. A metal frame work was made on the master cast for partial arches.
Occlusal rims were made on the temporary record bases or metal frame works, to record the relationship between the maxilla and mandible. Teeth were arranged according to the recorded jaw relationship. Trial dentures were checked in the participants' mouths and dentures were constructed with heat-cured acrylic resin (Acron Duo, Associated Dental Products Ltd., Kemdent, Wiltshire, UK) by a conventional denture-making procedure. After deflasking, the dentures were finished, and polished.
Participants were followed-up at T2, T3, T4, and T5. The clinician assessed whether there was any denture-related mucosal irritation due to the denture and where the denture-related mucosal irritation was localised. In order to eliminate mucosal irritations caused by the denture, the intaglio surface and the borders of the denture bases were continually re-adjusted. Prosthesis were made and controlled by a prosthodontist. Laboratory procedures were done by an expert technician.
Data were analyzed with the SPSS software package (Version 22, IBM SPSS Statistics, IBM Corporation, Armonk, NY, USA). Descriptive statistical analyses were performed with chi-square test, Freeman-Halton extension of Fisher's exact test and repeated measures one way ANOVA test where applicable. All tests were performed with 95% confidence for the determination of any statistical difference (P<.05).
RESULTS
Eleven of the 130 participants (9 females) were unable to tolerate the impression procedure. Nine participants (all females) started but did not complete the treatment and were omitted from the study. A total of 110 participants completed the restoration procedure. Flow chart of the study is given in Fig. 1. The characteristics of the participants are summarised in Table 2 (N=110) and the types of the mandibular removable partial dentures are given in Table 2a (N=44). A total of 17 participants could not use dentures after insertion; one patient refused the denture because of its smell, and 16 participants refused dentures because of gagging. All of these 17 participants opted for implant treatment. A significant correlation was found between gender and education level. The number of females who had completed only a primary school was significantly higher than males. Details are shown in education Table 2b (chi-square 17.679, P<.05).
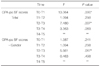
The mean GPA-pa SF scores for participants at T0 was 1.84 which decreased to 1.64 by T4 and was the same at T5. According to repeated measures one way ANOVA test significant difference was present between the GPA-pa SF scores (F=17.291, P=.000) and this difference changed significantly among genders (F=5.262, P=.006). This difference resulted from T0-T1 and T2-T3 scores in the case when the effect of gender was eliminated. Besides, the difference in the scores obtained for T2-T3 was significant among females and males (P<.05). Details for these results are given in Table 3a and Table 3b.
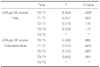
According to repeated measures one way ANOVA test significant difference was present between the GPA-pa SF scores (F=3.309, P=.014), however this difference was not significant according to education level (F=1.212, P=.293). According to this, significant difference was present between the mean scores obtained at T0 and T1 periods in the case when the effect of education was eliminated. (P<.05) Details for these results are shown in Tables 4a and 4b.
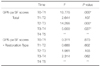
Denture-related mucosal irritation was seen in 52 participants (47.3%). Denture-related mucosal irritation was localised at the vestibule sulcus (24.5%), postdam area (18.2%), retromolar region (12.7%), alveolar ridges (9.1%), lingual sulcus (8.2%), mylohyoid line (8.2%), and mid-palatal area (2.7%). Participants with denture-related mucosal irritation due to denture use had higher GPA-pa SF scores compared to those without such denture-related mucosal irritation. Repeated measures one way ANOVA test revealed significant difference between the GPA-pa SF scores (F=30.482, P=.000) and significant difference was found among participants with denture-related mucosal irritation compared to those without such denture-related mucosal irritation (F=20.551, P=.027). According to this significant difference was present between the GPA-pa SF scores obtained at T0-T1, T2-T3 and T3-T4 in the case when the effect of denture related mucosal irritation was eliminated. Besides scores obtained at T3-T4 differed significantly in the presence of denture related mucosal irritation (P<.05). Details of these results are shown in Table 5a and Table 5b.
Five groups of removable dentures were evaluated. Participants with complete maxillary + partial mandibular dentures, partial maxillary + complete mandibular dentures, or only maxillary denture (partial or complete) had higher GPA-pa SF scores in all periods. Repeated measures one way ANOVA test presented significant difference among GPA-pa SF scores (F=10.035, P=.000). However, the dentures type did not have a significant impact on the GPA-pa SF score in any period (F=1.362, P=.157). According to this significant difference was present between the GPA-pa SF scores obtained at T0-T1, T2-T3 and T3-T4 in the case when the effect of dentures type was eliminated (P>.05).
DISCUSSION
Mean GPA-pa SF scores differed among the different periods of prosthetic restoration, with the highest score obtained before starting the restoration procedure. The decreasing of the GPA-pa SF scores with time could be related to several factors. A patient with complete dentures may develop a gagging problem due to the denture itself10 or psychogenic factors.7,9,10 When a denture of the postdam area extends to the soft palate, the most common factor leading to gag reflex is tactile stimulation of the sensory receptors of the soft palate. The patient may refuse to swallow saliva because of a fear that the denture will dislodge. As a result, saliva can accumulate and trigger the gag reflex.10 According to Fiske and Dickinson,7 experiencing something unpleasant before or during dental treatment may indirectly contribute to an exaggerated gag reflex. Similarly, Ramsay et al.9 suggested that participants with bad prior dental experiences will approach dental treatment with bias, and will behave the same during similar episodes in the future. Thus, gag reflex may be inevitable when something is placed in the mouth, or even at the thought of something being so placed.
In patients with removable dentures, mucosal irritation on oral tissues may also affect the gag reflex. Participants with denture-related mucosal irritation had significantly higher GPA-pa SF scores compared to those without this finding. In order to eliminate mucosal irritations caused by the denture, the intaglio surface and the borders of the denture bases were re-adjusted throughout the control period and a corresponding decrease was observed in the gag reflex. It was reported that negative impacts on physical function were caused by the denture in the mouth not sitting firmly as well as by problems caused by the sense of having something in the mouth leading to gagging, pain, soreness and bulkiness.14 In addition, ill-fitting dentures were reported to be related to gagging.7 Our results could be related to this previous observation; as denture-related mucosal irritation decreased over time, the adaptation and retention of the dentures improved, and participants became more comfortable using their prostheses and experienced less gagging.
According to our clinical experience and report of participants, denture-related mucosal irritation in the mouth during chewing could cause loss of adaptation and stability of the dentures, leading to gagging. Upon experiencing denture-related mucosal irritation or pain during chewing, the patient may slide their lower jaw to prevent pain. As a result, the adaptation and retention of the dentures are lost, and the denture detaches from the alveolar ridge, which may cause gagging.
Female participants had higher scores in all periods of restoration. Akarslan and Bicer8 reported that females had higher scores on the GPA-pa SF and higher dental anxiety scores on the Modified Dental Anxiety Scale (MDAS). Mohammed15 reported that females showed a higher incidence of gag reflex than males and attributed this result to women having relatively smaller jaws and being psychologically more sensitive when compared with males thus leading to an exaggerated gag reflex. Females typically report higher overall levels of dental fear compared to males.16,17
Education level was found to have no impact on the GPA-pa SF scores in any time periods analysed in the present study. Randall et al.18 found no correlation between gender, age or education differences in incidents of gagging in the dental clinic. Saita et al.19 reported that gagging problems were more frequent in males than in females.
The number of participants with a low education level was relatively high in this study. In Turkey, the education level is related to income.20 Generally, participants with a low education level earn less income than those who have higher levels of education. Participants with lower education levels (low income) may prefer university clinics for their dental treatments, whereas more educated participants prefer private clinics. The participants in this study were also predominantly female (70%), consistent with previous studies in which most removable denture users were female.21,22 Elderly females have more missing teeth and, therefore, are most in need of prosthetic treatment.23 Leles et al.23 reported that females had greater aesthetic expectation compared to males. Sociocultural and economic variables have relevant impacts on participants' attitudes towards treatment.
Although a significant difference was not present, participants with complete maxillary + partial mandibular, partial maxillary + complete mandibular, or only maxillary (complete or partial) dentures had higher GPA-pa SF scores in all periods. To our knowledge, no similar study has been performed to which we can compare our findings. Nevertheless, Murphy24 reported that the gag reflex was most aggravated in participants wearing complete maxillary dentures, followed, in order, by partial maxillary, complete mandibular, complete maxillary + mandibular, and partial mandibular dentures. The difference between our findings and those of Murphy may be related to differences in the classification of the restoration types and the description of data between the two studies. We used the GPA-pa SF and repeated measures one way ANOVA test, whereas Murphy used only descriptive statistics of the participants in his study.24 It was reported that the distolingual region of the mandibular dentures can irritate the trigger zones and produce gagging.25 In this study, most of the participants used mandibular dentures with distolingual extension.
Questions from the standard form, including those of the GPA-pa SF, were read aloud to participants. This format may be prone to bias, influencing the results regarding gag reflex. This limitation should be considered during the evaluation of the results obtained from this study.










 XML Download
XML Download