

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In recent years, the prefabricated fiber-reinforced composite post has become popularly used for the direct post and core restoration due to their good esthetics and relatively low elastic modulus.1,2,3,4 The combination of fiber-reinforced composite post and composite resin core produced the lower stress concentration in any part of the restored endodontically treated teeth when compared with other post and core materials,5 resulting in a lower incident of root fracture. The long term study of failure of composite posts showed much lower failure rate than metal posts.6,7,8 However, the fit of the fiber post in the intra-radicular dentin is not as precise as that of conventional cast posts. Therefore, the retention of fiber posts is usually obtained from resin cement in combination of an adhesive system.9
The dual-cured resin cements have been employed to bond fiber posts in a root canal due to the combining self-cured and light-cured capability. However, several studies reported the light-cured mode to dual-cured composite showed higher micro-tensile bond strength to dentin, rather than the self-cured mode.10,11 Therefore, the bond strength of resin cement employed to bond fiber posts in a root canal depends on sufficient light transmission through the post.
Modern prefabricated fiber-reinforced composite posts are made of white or translucent fibers such as glass, quartz or zirconia fiber. Some of these posts have been reported to transmit light along the post, leading to a higher initial polymerization of resin cement. Several studies have described the ability of light transmission through several types of composite posts with several techniques such as direct measuring by photometer,12,13 indirect micro-hardness test14,15,16 or direct FT-Raman spectrometer17 to evaluate the degree of conversion for resin cement cured through the light-transmitted post. All studies concluded that the quantity of light transmitted depends on the resin matrix and the fiber composition of each post. However, most studies recommend using FTIR methodology to directly evaluate the degree of conversion on the cement.12,13,14,15,16 Faria e Silva et al.17 employed the Fourier Transform Raman (FT-Raman) spectrometer which is a more accurate method to evaluate the degree of conversion for resin cement cured through the post. They used the dual-cured resin cement for their evaluation which influences the degree of conversion by chemicals. To avoid the effect of chemical influence in dual-cured resin cement, the light cured composite was used in this study.
Therefore, to enhance the bond strength of the post to dentin by light cured mode, the information of the depth of light transmission through a translucent fiber post is necessary. The objective of this study was to evaluate the depth of cure of resin composite cured by light through a translucent fiber post. The null hypothesis was that there are no significant differences among the degree of conversion of the composite along the entire depth and surrounding area 1 mm apart of a translucent fiber post.
MATERIALS AND METHODS
D.T. light-post (RTD, Saint Egreve, France) and FRC Postec Plus (Ivoclar Vivadent AG, Schaan, Liechtenstein), reportedly light transmitted posts, were used as the experimental posts in this study. The detailed information of the posts was shown in Table 1. D.T. light-post No. 2, 18 mm length, tapered posts with maximum and minimum diameters of 1.8 and 1.0 mm and FRC Postec Plus No. 3, 20 mm length, tapered posts with maximum and minimum diameters of 2.0 and 1.0 mm were selected for use in this study. The posts were initial cut at the top of the post to the same length at 16 mm. The dimensions of the posts and cutting portions were shown in Fig. 1.
The opaque plastic tubes with diameter of 5 mm were cut in various lengths of 2, 4, 6, 8, 10, 12, 14 mm. The prepared post was longer than the highest plastic tube by 2 mm. The other lengths of the posts were cut at the apical tip in increments of 2 mm to match the other lengths of the plastic tubes, respectively (Fig. 2). The composite resin (Filtek Z350, shade A3, 3M ESPE, St. Paul, MN, USA) was filled in plastic tubes then the posts were aligned with acrylic aligner box and put in the center of composite in plastic tubes. The top was covered with opaque plastic sheet before light curing. The composite was cured by light using a Elipar-Freelight 2 LED light curing unit (3M ESPE, St. Paul, MN, USA) with wavelength 430-480 nm, intensity 1000 mw/cm2. The 8 mm light tip was placed in contact with the post tip to activate the polymerization of the composite for 40 seconds on standard mode as recommended by the manufacturer.
The bottom surface of the cured composites were then examined for the degree of conversion (DC) using a Fourier transform infrared spectrometer (OMNIC 6.1, Nicolet Instrument Corp, Madison, WI, USA) in attenuated total reflection (ATR) mode (ZnSe crystal) for three positions at 0.1, 0.5 and 1.0 mm apart from the post surface under microscope. The schematic diagram of the specimen preparation was shown in Fig. 2. The upper surface of the specimen which was cured by the direct light without opaque plastic sheet was examined as positive control. The uncured specimen was also examined as negative control. The specimens for all conditions were repeatedly prepared and tested for four times (N = 4). The spectra of the cured and uncured were obtained using 128 scans at a resolution of 4 cm-1, at the range from 1000 to 6000 cm-1 was scanned. The spectra were subtracted the background spectra out using FTIR machine provided software (OMNIC 6.1, Nicolet Instrument Corp, Madison, WI, USA). The acquired spectra were expanded and analyzed in the region of interest from 1560 to 1670 cm-1. The degree of conversion (DC) was calculated by standard baseline technique using the comparison of peak area at 1639 cm-1 (aliphatic c=c) and internal standard peak at 1609 cm-1 (aromatic c=c). The DC was calculated by the following equation:

The results of DC were analyzed by three-way ANOVA and Tukey's tests.
RESULTS
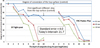
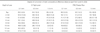
The degree of conversion of resin composite at 0.1 mm, 0.5 mm, and 1.0 mm from the post surface of the seven depth levels for each type of post, were shown in Table 2 and Fig. 3.
The results of ANOVA in Table 3 clearly showed that the degree of conversion of the composite depends upon all three main factors which were type of post, depth along the post and distance apart from the post and their interaction. The post-hoc Tukey's test showed the different interval at 21.7 (P=.05).
The resin composite around both D.T. light-post and FRC Postec Plus showed the highest degree of conversion at the 2 mm level of all area apart from the post surface and continuously decreased when the distance from the light source was increased. For each level, the highest degree of conversion was at 0.1 mm from the post surface and decreased continuously when the distance apart from the post surface was increased.
The degree of conversion of 0.1 mm from the post surface of D.T. light-post slightly decreased according to the increase of depth level differed from the others.
From Fig. 3, the average line of the degree of conversion of the top surface (positive control) and the first statistical significant different step line compared to the control (Tukey's interval =21.7, P=.05) were drawn. From these two lines found that the degree of conversion of the composite cured by light through DT light post up to 6 mm depth except 1mm apart from post of 6 mm depth were not difference from the control (P<.05). For those of the FRC postec Plus, only 0.1 and 0.5 mm apart from post at 2 mm depth were not difference from the control (P<.05).
DISCUSSION
In this study, we selected to evaluate only two brands of the translucent fiber post as a representative of different resin matrices, using FTIR/ATR methods. The composite resin was chosen instead of resin cement in order to minimize the effect of chemicals cured on dual cured process. Although this study may show little clinical relevance due to the use of dual cured resin cement to bond the post rather than using light cured composite, This experiment was set up to fulfill the objective of checking how deep the light can transmit along the post.
The results clearly showed the degree of conversion of the composite depends upon all three main factors which were type of post, depth of post and area apart from the post surface, and their interaction. The decreasing pattern of degree of conversion of both posts was nearly the same in terms of the depth from the top of the post and distance apart from the surface of the post. The degree of conversion was decreased when the depth and distance apart from the post surface increase and drastically decrease when the depth from the top of the post was greater than 6 mm. This data conformed to several studies that the light transmitted through the post was drastically decreased when the depth from the top of the post more than 4-6 mm13,14,15,16 and showed insufficient transmission of light to polymerize the resin cement or composite.15,16 This means that in clinical situation, the expectation of light-cured mode of resin cement cannot be expected especially in deeper part more than 4-6 mm and also the area apart from the post. Moreover, it is almost impossible to use the light transmitted post to carry the light to cure the light activated resin or composite in any clinical situation.
However, the D.T. light-post showed two different points of degree of conversion pattern compared with FRC Postec Plus. Firstly, at the initial degree of conversion at 2 mm depth, the D.T. light-post was slightly higher than FRC Postec Plus in any distance apart from the post and secondly, at 0.1 mm apart from the post of D.T. light-post showed slightly decreasing pattern compared with those of FRC Postec Plus. These differences seem to depend on the resin matrix rather than on fiber composition of the post. The fiber composition of these two posts was not much different. D.T. light-post used Quartz and FRC Postec Plus used glass as a fiber of the post. These two fibers have nearly similar light transmission characteristics.18 However, the resin matrix of these two posts was much different. D.T. light-post contains only epoxy resin as a matrix while the resin matrix of FRC Postec Plus contain UDMA and TEGDMA as a core and several modified additives such as Ytterbium trifluoride, a highly dispersed silicon dioxide. These additives may have influenced the light transmission due to their white opaque color.
CONCLUSION
Within the limit of this study, it can be concluded as below.
The quantity of light transmission depends on type of post.
The quantity of light transmission reduces as the depth and the distance apart from the post increased.
The light transmission capability of the post is insufficient for clinical light activation of resin.




 XML Download
XML Download