This study is a photographic evaluation of the border of the tragus to be used to form Ala-tragal line in orthognathic dentate subjects. The photographic technique used in this study is non-invasive and simple and the entire technique was standardized. The subject-to-camera distance (1.5 m) was set at approximately 10 times the maximum breadth of the subject (approximately 15 cm from ear to nose) reduces photographic distortion to less than 1%.
13 With respect to the angular measurements from 2-dimensional image of a 3-dimensional object, 3 types of errors may arise.,
14 namely; errors of projection, mechanical errors in drawing lines between points and errors of land mark location. Projection error is reduced by the use of angular measurements because the values of angular measurement remain constant regardless of the enlargement factor. Errors introduced in drawing and measuring lengths and angles by hand can easily be eliminated by machine computation, as done in this study, provided that the reproducibility of digitization of individual points is high. Precise positioning of the subject, especially with no external device is very difficult, resulting in a situation in which the true anatomic mid-sagittal plane coincides with the nominal mid sagittal plane at the focusing plane only rarely and by chance. To minimize this error, in the study, a plumb line was suspended in front of the mirror that was used to bisect the facial refection and to minimize lateral head rotations. This also served to standardize the mid-sagittal plane to film distance. The points that have to be digitized on the photographs are clearly defined to minimize the intraexaminer location error. Photographs were taken with the subjects positioned in the natural head posture (NHP). NHP is a logical orientation adopted for assessing facial profile as it relates to the patient's head posture in daily life. Subjects' natural posture was used as against a cephalostat to position the patients, as insertion of ear posts could itself be argued as positioning the subject unnaturally. Sutcher & Eliasson had concluded that insertion of ear posts altered the position of the condyle within the fossa and perhaps this could result in proprioceptive feedback altering the action of the muscles maintaining head posture.
15 The Eye-Ear plane (EEP) i.e. OT
1 which is comparable to Frankfort horizontal plane (FH plane) is taken as a standard reference plane as it is (FH plane) stable and is not affected by tooth loss. Also it is universally accepted as a fixed cranial plane.
16 The subjects were selected between the age group of 18-40 years. By 18 years growth of the face ceases and there is no change in the relationship of camper's plane to the occlusal plane. The upper age limit was restricted to 40 years as at this age a dentition can be expected to remain normal without tooth loss and excessive attrition. For the ease of the comparison of the angulations, only orthognathic subjects were selected in this study.
10 The angulation of the occlusal plane to the FH plane (OT
1) is known as "cant of the occlusal plane" and was first enunciated by Downs.
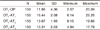
17 The mean cant of the occlusal plane (OT
1-OP) as determined in this study is 11.96, which is comparable to the study done by Hartono
18 who in case of normal type found to be 12°.
Table-I shows that mean angle of OT
1-AT
3 (10.3167) is close to mean angle of OT
1-OP (11.9651) i.e. the angle formed between FH plane and occlusal plane is closer to the angle between FH plane and ala-lower border of the tragus. This means that the occlusal plane is more parallel to the line drawn from the ala to the lower border of the tragus. This is in accordance with the studies done by Clapp
6 (1910), Dalby
6 (1912), Wilson
6 (1917), Hartono
18 (1967), van Niekerk
19 (1985) and Karkazis and Polyzois
5,
20 (1986). They found out that the occlusal plane is parallel to the line drawn from the lowest point of the ala of the nose to the lower border of the tragus. The occlusal plane, as established by tooth arrangement should be located according to mechanical requirement for stability of denture and preservation of the supporting structures. It has been found (Nagle and Sears
8-1962 & Swenson
21-1947) in case of excessive resorption, the plane should be placed closer to the resorbed ridge to reduce the leverage. It should be perpendicular to the forces of mastication and should be developed parallel to the lower ridge. As the occlusal plane is parallel to the lower border of the tragus than the middle and superior borders the forces of mastication will be perpendicular to the occlusal plane and there will be less leverage on the lower residual ridge which is most commonly involved in resorption process (Jacobson and Karol
6-1983) and results in denture stability. The occlusal plane placed high in relation to lower ridge result in additional leverage and denture instability (McGee
22-1960). In this study comparison between angles OT
1-OP (FH plane and occlusal plane) and OT
1-AT
3 (FH plane and ala to lower border of tragus) which is 1.6484, found to be close to the comparison between angles OT
1-OP and OT
1-AT
2 (i.e. between FH-plane and occlusal plane angle and FH-Plane and ala-to middle border of tragus angle) 1.7093 (
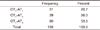
Table 1). This was due to the length of the Tragus. In the subjects with short tragus there was not much distance between lower and middle border of the tragus thus making both the lower and middle border almost parallel to occlusal plane. Length of the tragus was measured in these subjects. It was found that out of the 26% subjects showing occlusal plane parallel to line connecting ala to the middle of the tragus, in comparison 16% of the subjects had small tragus with very small distance between middle and lower border of tragus. Thus, these 16% subjects can also be included in subjects showing occlusal plane parallel to the line joining the ala to the lower border of tragus. It is found that there is no influence of the sex on the level of occlusal plane i.e. both males and females showed the occlusal plane parallel to the line joining the ala to the lower border of tragus. In this study it was found that in 20.7% of the subjects' upper border of the tragus is parallel to the occlusal plane, in 26% the middle border of the tragus and in 53.3% the lower border of the Tragus (
Table 3). This might be due to the anteroposterior dimensions of the maxillary base, which governs angulation of the occlusal plane. The greater the distance between ANS (anterior nasal spine) and the hamular notch i.e. wider anterior cranial base, the more acute the angulation of the occlusal plane and conversely, the smaller the distance the more obtuse the angle will be. This is given by Sloane and Cook.
23 This tendency has been confirmed by the cephalometric studies of L' Estrange and Vig
24 and represents a phenomenon that may be explained by the "denture glass effect". It might also be due to the fact the steepness of the curvature of occlusal plane varies in different individuals and frequently a noticeable difference may be observed in the plane on the two sides of the arch in the same individual.
25
As the prosthodontic intervention imposes most of its influence of the denture stability, due importance must be given in analyzing the occlusal plane level, which is the main contributing factor in denture stability. The position of the occlusal plane of orientation also forms the basis for ideal tooth arrangement and fulfills the necessary mechanical, esthetic and phonetic requirements and aid respiration and deglutition. Standard facial measurements are essential for establishing the level of occlusal plane. However, occlusal plane level analysis data apply to the ethnic group from which they are obtained. Data from one ethnic group may be misleading when applied to other ethnic group as different racial groups have different facial characteristics. Therefore, care must be taken when the norms found in standard textbooks are applied to non-Caucasian racial groups.


 PDF
PDF ePub
ePub Citation
Citation Print
Print






 XML Download
XML Download