

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
To establish occlusal plane while recording maxillomandibular relation during fabrication of complete denture, many methods have been tried in the past. However, none of these methods proved its accuracy to perfection. Needless to say that correct orientation of the occlusal plane plays a vital role in providing optimal esthetic and functional satisfaction.1 Improper orientation of this plane jeopardizes the coordination between the components of Oro-Facial Articulatory Complex.2
The plane of occlusion is formed after joining the incisal edges of the mandibular central incisors to the disto-buccal cusps of the mandibular first molars. The occlusal plane is defined as the common plane established by the incisal and occlusal surfaces of the teeth (Glossary of Prosthodontic Terms-8). It is not a plane in the true sense of the word, but represents the mean of the curvature of the inciso-occlusal surfaces of teeth.
There is a controversy for the orientation of the occlusal plane during complete denture fabrication. Various landmarks and techniques had been used over the years by clinicians and researchers for establishing this plane which include:
Establishing the occlusal plane according to aesthetic requirements anteriorly and parallel to the ala-tragus line posteriorly (Craddock,3 1951; Schlosser & Gehl,3 1953), positioning the occlusal plane parallel to and midway between the residual ridges (Nagle and Sears,3,4 1962; Boucher et al.,5 Boucher6 1964), orientating the occlusal plane with the buccinator grooves and the commissure of the lips (Lundquist and Luther,7 1970), Terminating the occlusal plane posteriorly at the middle or upper third of the retromolar pad (Ismail and Bowman,8 1968), positioning the occlusal plane on the same level as the lateral border of the tongue (Ismail and Bowman,8 1968 ; Yasaki,9 1961) and many more concepts are reported in literature.
However, the most acceptable method of orienting the occlusal plane is to make it parallel to the ala-tragus or Camper's line as reported in several modern text books. In spite of its widespread acceptability, it is surprising to note that the exact location of the point on tragus while marking ala-tragus line is unclear. This has created lot of confusion while selecting a point for marking ala-tragus line. So this study was therefore undertaken to decide the most appropriate point on tragus to be used as a reference point while marking ala-tragus line.
MATERIALS AND METHODS
This study was carried out using simple and economical instruments and materials.
For the study, following two devices were custom-made.
1. The occlusal plane analyzer(OPA)(Fig. 1) was developed to verify the parallelism of the occlusal plane of maxillary occlusal rim with ala-tragus line in posterior and interpupillary line in the anterior region. It comprises of lower plate having outer "U" shaped frame which will be located over the face and Inner fork plate having a shape of average arch. Three metal Scales having holes at both the ends to pass through four threaded vertical rods - two lateral scale and one Frontal scale and these scales can be adjusted and fixed at a desired height on vertical rods using nuts to simulate parallelism of the occlusal plane with ala-tragus line and interpupillary line.
The lower plate was made of stainless steel with a thickness of 1 mm. Four threaded vertical rods with the corresponding nuts were used to fix the lower frame with the upper two lateral and frontal plate at a desirable vertical height to check parallelism of the occlusal plane with ala-tragus line which was marked using Superior point on tragus with ala. The occlusal rim was positioned over the edentulous foundation and was supported by the fork plate of the lower frame. The maxillary occlusal rim was adjusted for: height, labial inclination and arch form. The occlusal plane was then adjusted to achieve parallelism - anteriorly with interpupillary, posteriorly with ala-tragus line (Fig. 2A). The metal foil was then adapted over the adjusted occlusal surface of the rim (Fig. 2B). The lateral scales were adjusted in line with the ala-tragus line and were fixed in position by tightening the nuts over the threaded vertical rods. The frontal scales was also adjusted at the level of interpupillary line and secured tightly in position using the nuts (Fig. 3) over the patient's face.
2. The transpar ent plastic angle measuring device:- Rectangular acrylic sheet (transparent) measuring 16 × 13 cm was used as a platform plate. Over this plate 3 plastic (transparent) scales were fixed (one horizontal at the bottom and two in lateral sides in such a way that the inner angles between these scales were exactly measured 90° (Fig. 4). This simple custom made device was used to measure various angles. The protractor was modified to obtain reading between 0-90°. This modified protractor has provided the opportunity to measure the angles between various planes used in this study. The transparency of this device offered clarity while measuring the angles by positioning it over the tracing line(s) of the cephalograph accurately.
Data was collected for two groups of the subjects: (A) Dentulous group, (B) Edentulous group having sample size of 30 for each group with equal gender distribution. Selection criteria for dentulous group includes -subjects aged between 18-30 years, having 28 to 32 teeth and ideal arch alignment with Angle's class I molar relationship, andno history of orthodontic treatment with normal profile. Selection criteria for edentulous group includes subjects aged between 50-70 years, havingh no history of TMJ disorder and associated pathology, neurological disorder and maxillofacial trauma with clinically healthy oral mucosa.
Three points were indentified on tragus of ear as Superior (S), Middle (M) and Inferior (M). The stainless steel balls (3 mm in diameter) were fixed at these selected points and also at the ala of the nose with fine quality double sided adhesive tape to ensure perfect placement to capture the recording on cephalographs (Fig. 5A). The patient was adjusted with Cephalostat as per standard procedure (Fig. 5B). Lateral cephalographs were then shooted, developed and fixed by using standard technique. For edentulous patients, the maxillary (wax) occlusal rim was adjusted forLabial inclination, Arch form, midline and canine lines were marked and occlusal plane was adjusted using occlusal plane analyzer (Anteriorly parallel to the interpupillary and posteriorly parallel to the ala-tragus line). Now this adjusted maxillary occlusal rim with adapted metal foil on the occlusal surface was positioned over the maxillary foundation. The ala-tragus line was marked by joining Superior point of tragus with base of the ala of the nose. The adapted metal foil was recorded as radio opaque line in lateral cephalographs. Similar technique was used to shoot the lateral cephlographs as in dentulous subjects.
The points used for tracing were Orbitale (Or), Porion-(Po), Superior (S), Middle (M), Inferior (I) point of tragusand Inferior point of the ala of nose (A). Various Planes marked were Frankfort horizontal plane (FH), Occlusal plane (OP) and three Planes formed by joining S to A (SA plane), M to A (MA plane) and I to A (IA plane). Various angles evaluated in this study were Cant of occlusal plane (COO), Angle between FH plane with SA plane (SFH), MA plane (MFH) and IA plane (IFH). The angles between OP plane and SA plane (SOP) MA plane (MOP) and IA plane (IOP)were also measured (Fig. 6).
Angle COO was used as a standard which is the angle formed between the FH plane and the occlusal plane.
In Downs analysis, the occlusal plane used was formed by marking a line bisecting the occlusal surfaces of permanent molars and incisal overbite. Mean value of angle COO was found to be 9.3° and ranges between 1.5° to 14° in those samples used in Downs study.10-12 This angle measures the slope of the occlusal plane relative to Frankfort horizontal plane.
Over the traced cephalographs of dentulous patient, the values of angles COO, SFH, MFH, and IFH were measured, tabulated and compared with the value of average COO angle from Downs Analysis. Along with this, the value of angles SOP, MOP, IOP were also measured and tabulated. On the cephalographs of edentulous subjects, the angle between FHP and SA, MA and IA was measured, tabulated and compared with the value of average COO angle from Downs analysis (Fig. 7).
The measurements recorded for dentulous and edentulous subjects were tabulated and subjected for the statistical analysis (Statistica- version 6, Stas.soft., Oklahoma, USA). Comparitive evaluation of the angles - COO, SFH, MFH, IFH, SOP, MOP, IOP in dentulous subjects and SFH, MFH, IFH in edentulous subjects were carried out to find out the significance and its usefulness in deciding the most appropriate point on tragus to be used as a reference point while marking the ala-tragus line. Statistical tests used were descriptive analysis, Student's unpaired t-test and Pearson's correlation coefficient.
RESULTS
After statistical analysis the results were tabulated and following results were drawn:-
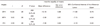
Table 1 (Dentulous group) demonstrated mean value of COO in male and female was 9.93 and 9.60, respectively. with average value of 9.76. Mean IFH in male and female was 11.20 and 9.60, respectively with average value of 10.40. The mean IOP in male and female was 2.26 and 2.66, respectively with average value of 2.46. The mean IFH was closest to mean COO and mean IOP was closest to 0° compared to the SOP and MOP.
In Table 2, the edentulous group shows that the mean IFH in male and female was 10.93 and 10.20, respectively with average value of 10.56. The mean IFH was closest to average COO 9.3°.
Correlation and Probability of COO with SFH, MFH, and IFH of the dentulous group was calculated and positive correlation was observed between COO and SFH, MFH, IFH. Student's unpaired t test exhibits the mean difference in means of SFH, MFH, IFH with COO found to be statistically significant SFH (P=.007), MFH (P=.005) and IFH (P=.007).
The mean angle of IFH in male was 11.2° with standard deviation of 2.45 and IFH in female was 9.6° with standard deviation of 3.13°, which is closest to average COO mean 9.3° compared to SFH and MFH. In Tables 3 and 4, it is noticed that the mean difference in mean angle was found to be statistically significant for SFH (t =14.90, P=.000), MFH (t = 9.65, P=.000), IFH (t = 2.99, P=.006) in male and for SFH (t = 12.37, P=.000), MFH (t = 5.88, P=.000) in female but Statistically insignificant for IFH in female(t = 0.37, P=.714).
The mean angle of IFH in male was 10.93 with standard deviation of 2.89 and in female was 10.20 with standard deviation of 3.42, which is closest to average COO 9.3° when compared to SFH and MFH.
Tables 5 and 6 demonstrate student's unpaired t test which shows that the mean difference in mean angle was found to be statistically significant for SFH (t = 13.24, P=.000), MFH (t = 5.52, P=.000), IFH (t = 2.18, P=.037) in female and for SFH (t = 11.56, P=.000), MFH (t = 6.93, P=.000) in female, but was statistically insignificant in female (t = ++1.01, P=.318).
DISCUSSION
Some of the existing concepts regarding orientation of the occlusal plane in the edentulous patients are of the opinion that the occlusal plane has relation with Camper's line. It is the oldest, simplest and most commonly used method. It would seem desirable to locate it accurately and propagate its use while establishing the occlusal plane.13 The definitions of the ala-tragus line has created confusion. The exact points of references on tragus and ala are not categorically specified.14 Spratley14 described it as running from the center of the ala to the center (middle) of the tragus. Boucher5,6 defines it as "The line running from the inferior border of the ala of the nose to the superior border of the tragus of the ear."
However, out of the seven texts that propound its use, only one has provided proper definition and it cites Boucher's5,6 definition. Two texts recommended the concept without defining or illustrating it, while three provided only pictorial representation. The latter are of immediate concern, for in each illustration; Camper's line is clearly depicted as extending to a point, not at the superior border, but at the center of the tragus of the ear. This pictorial representation corresponds to the definition given by of Ismail and Bowman8 (1968) and evidently reflects an understanding of the concept, which predates Boucher's definition.15
Camper's plane is defined as (i) a plane established by the inferior border of the left or right ala of the nose and the superior border of both ears; (ii) a plane passing from the acanthion to the centre of the bony external auditory meatus (GPT 1999). The occlusal plane is considered to be parallel to this plane.15
In this study, the widely accepted Downs analysis10 was used as a base line for comparison. Downs analysis on variations in facial relationship indicates that the cant of the occlusal plane (COO), the angular relation between the occlusal plane and the Frankfort plane, ranged from 1.5° to 14° with a mean value of 9.3°.10-12
The Frankfort horizontal plane is a fixed anatomical craniometrical landmark, thus being used as a skeletal guideline while locating occlusal plane posteriorly.16 It has no effect of the loss of teeth and it can be easily located with the help of lateral cephalograph and therefore FH plane was used in this study.
The mean value of COO was observed to be 9.7° in this study which is within acceptable range of 1.5° to 14° and closest to mean value of 9.3° as demonstrated in the Downs study. The difference of 0.4 degree is clinically insignificant and may be accredited to the variations in racial population.
The mean angle (total) IFH found in dentulous subjects and edentulous subjects was 10.40° and 10.56, respectively. Thus, the mean value of IFH angle is comparable with the mean value of the angle established in Downs analysis.10-12
The mean angular value of IOP 2.46 ± 2.48°, is least among SOP and MOP. This observation of the present study is similar to the observation of van Niekerk et al.15 (1985) who recorded an angle between the occlusal plane of complete dentures and the ala tragus line (inferior point on tragus was used) as 2.45° (SD = 3.24). This means that the line marked from the inferior point of tragus to ala of nose was the most parallel line with the occlusal plane in dentulous subjects as compare to the lines from superior and middle point of tragus with ala of nose. This underlined the importance of using "Inferior point" for marking ala-tragus line during recording of jaw relation for edentulous patient. The results of this study are in agreement with the previous studies by Clapp13 (1910), Dalby13 (1912 and 1914), Wilson13 (1917), Giffen13 (1925), Gillis13 (1933) and Hartono17 (1967).
The statistical analysis carried out for males and females for the various angles in dentulous and edentulous, males and females shows no significant difference (P >.005). This indicates that gender difference does not cause any variations in the angular relationship between the ala-tragus line and Frankfort horizontal plane and alatragus line and occlusal plane. Therefore it was concluded that inferior point on the tragus is the most valid point for males as well as female while marking ala-tragus line for establishing occlusal plane. In accordance to the results obtained in this study the order of preference out of three tragus point for marking ala-tragus line is inferior point (I), middle point (M) and superior point (S).
It is also observed that when posterior occlusal plane was established using ala-tragus line marked from the superior or middle point, the occlusal plane was placed at a higher position which is in agreement with the results of the previous studies.2,5,6,18-22 But, it is contrary to the study of Nissan et al.23 where superior point on tragus was recommended. The middle point on the tragus was also recommended as a point for establishing occlusal plane in some studies.13,21,24-26 These variation may be due to effect of racial and ethnic populations.
The values of SFH, MFH, IFH this study for both dentulous and edentulous subjects confirms that the inferior point gives closest value of COO closer to Downs analysis. Statistically significant difference was observed between average COO and mean angular values of SFH, MFH, IFH for all groups, except for IFH values for female in both dentulous (P=.714), and edentulous (P=.318) group where there was no significant difference found. Therefore, as indicated by the results of this study, the inferior point in females gives closer angle with FHP, to average value of COO.












 XML Download
XML Download