

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Revolutionary changes in the field of dentistry have been made possible by the combined use of computer-aided design and computer-aided manufacturing (CAD/CAM) technologies and scanners. Digital data of oral tissues can be directly utilized in design and manufacturing procedures, meaning that the production of prostheses is possible without the use of conventional materials and procedures. Digitization of oral tissues can be performed intra-orally by the direct scanning of oral tissues or extra-orally by scanning either models or impressions of oral tissues. The scanning of impressions has the advantage of eliminating the model fabrication procedure, which is both time-consuming and a potential source of error. However, it has been relatively under-used compared to other scanning modalities because of the elastic property of impression materials and scanning accessibility problems caused by the complex shape of the negative replicas. Three types of scanners are typically used in this field: Mechanical scanners with a touch probe, laser scanners, and white light scanners,1,2 the most recently developed white light scanners show some features, which are advantageous for the scanning of impressions. As light scanners work without touching or pressing objects, the risk of deformation of elastic impressions may be decreased compared to mechanical scanners.1 The performance of white light scanners is reportedly higher than that of laser scanners,2,3 because white light scanners analyze multiple stripe pattern,3 while laser scanners analyze a line pattern. While there are numerous investigations looking at scan performance on tooth models,1-9 studies of scan performance on impressions are scarce. Quaas et al. examined the performance of a touch-probe digitizer and concluded that mechanical digitizing cannot be recommended for the direct digitizing of dental elastic impressions.10 Persson et al. reported a discrepancy of less than 40 µm when comparing digitized impressions made with a laser scanner with the stone replicas.8 Few previous studies have examined scan performance with regard to repeatability, and there is, therefore, insufficient evidence to support the use of these methods in clinical practice. Furthermore, there is one report on the performance of white light scanners for the polysiloxane impression material.11 However, no studies have confirmed the repeatability corresponding to silicon rubber impressions of abutment teeth type. Therefore, we aimed to evaluate the repeatability of the digitizing of silicon rubber impressions of abutment teeth using a white light scanner and compare differences in repeatability between different types of abutment teeth.
The hypothesis of this study was that there was no difference in repeatability of scanning values among silicon rubber abutment teeth impressions.
MATERIALS AND METHODS
Plastic tooth models of 3 representative types of upper teeth including the right canine, right first premolar, and right first molar were selected (AG-3, Frasaco, GmbH, Germany). A dental CAD/CAM system (Intellifit™ dental restoration system, SensAble Technologies Inc., MA, USA) with a haptic device (SensAble PHANTOM® Desktop™, SensAble Technologies Inc., MA, USA), device for reading the 3-dimensional shapeis allowed to make direct contact with an apparatuspencil, which was used to recreate typical abutment tooth shapes. After scanning these tooth models, the haptic device performed preparation of abutment teeth providing axial clearance of 1 mm, occlusal and incisal clearance of 1.2 mm, an axial wall angle of 5°, and a deep chamfer margin design. The CAM system (DT400, Doosan Infracore Co., Ltd, Seoul, South Korea) was used to create titanium abutment teeth models using the milling machine to minimize abrasion during the impression procedure.
Impressions of the prepared titanium abutment teeth were fabricated using extra-light body of a silicon rubber impression material (Aquasil Ultra, Dentsply, St. York, PA, USA) used individual plastic band (Fig. 1). The white light scanner (Identica®, Medit, Seoul, Korea) equipped with 2 digital cameras that are placed at an angle of 15° to the object table were used in this experiment (Fig. 2). Before the scanning procedure, the impression body was fixed on the table inside the white light scanner and the table was moved automatically in order to achieve the appropriate angles to obtain complete images. Various 3D images obtained from different angles were repeatedly rearranged and combined to get the complete 3D shape data of a stereolithography (STL) file format. Unnecessary parts of data including data from beyond the finishing margins, which seemed to be inaccurate, were deleted.7 The scanning procedure was repeated 8 times for each type of abutment tooth. Data from the first scan of each tooth type were used as the reference model, and the remaining 7 scans were compared with the designated reference model. Before the comparison, 7 scans excluding the reference model were converted from STL format into the point cloud-ASCII format using the CopyCAD 7.350 SP3 (Delcamplc., Birmingham, UK). The reference model was aligned as a 3D-surface model and was superimposed with the point cloud data of the other scans using the PowerInspect 2012 (Delcamplc., Birmingham, UK). Discrepancies between the 2 were measured and displayed as color-difference maps (Fig. 3, 4 and 5). After filtering the data, the amount of discrepancy of the whole tooth surface was measured in the form of absolute values. Mean and standard deviation (SD) of the overall discrepancy for 3 types of abutment teeth were calculated and statistically compared using the nonparametricKruskal-Wallis test with post-hoc pairwise comparison by the Wilcoxon rank-sum test, applying an adjusted alpha level (0.17 = 0.05 over 3, number of comparisons). All the statistical procedures were performed with SPSS version 20.0 (SPSS Inc., Chicago, IL, USA). In addition, a qualitative analysis was performed to produce the color-difference maps for canine, premolar and molar. Point numbers 2095, 2071 and 3803 were selected from the point cloud for the quantitative analytic procedure. These were filtered by an interval of 15 µm among all the points of scanned point cloud 26037, 24567 and 44702 for the canine, premolar and molar teeth, respectively. The color-difference maps allowed qualitative visual assessment, where green points indicate an exact fit, a positive discrepancy (greater than the reference model) is shown as yellow or red points, and a negative discrepancy (smaller than the reference model) as turquoise or blue points (Fig. 3, 4 and 5).
RESULTS
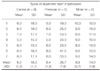
Table 1 shows the means and standard deviations of the 7 scans for the 3 types of abutment teeth impressions (n = 8 per type). The means of the discrepancies for each tooth type were 6.2 µm (95% confidence interval [CI], 5.4-7.1), 6.4 µm (95% CI, 5.2-7.6), and 8.8 µm (95% CI, 8.2-9.4), for the canine, premolar and molar teeth, respectively. The mean discrepancy of the molar scans was significantly higher than those of either the canine or premolar scans (Table 2). The variation in discrepancies (as mean [SD]) in the scans of the premolar tooth, which had a relatively longer axis and smaller diameter, were significantly larger than variation in the scans of the canine and molar teeth: 26.7 µm (95% CI, 19.6-33.7); 16.2 µm (95% CI, 15.2-17.3); and 14.0 µm (95% CI, 12.3-15.6), respectively.
As a qualitative analysis, color-difference maps were investigated. The color-difference maps of the canine scans were predominantly green indicating an exact fit between scans and the reference model; however, red or blue colors, indicating positive or negative discrepancies, can be seen on the labial surface of some scans (especially A and B), and the axial surface of most canine scans (Fig. 3). In maps of the premolar scans, though most of the occlusal surface is green, an area of blue and some red is seen, particularly in the axial wall region (Fig. 4). Similarly, whilst the maps of the molar scans are generally green, some blue or red is seen on the axial surface (Fig. 5).
DISCUSSION
These findings demonstrate excellent repeatability of the white light scanner in digitizing of silicon rubber impressions of 3 representative types of abutment teeth-canine, premolar and molar. The low mean discrepancy, ranging from 6.3 µm to 8.8 µm, is much smaller than those in previous reports. For example, mean positive deviations between 27 µm and 28 µm were achieved with mechanical digitization of an impression body using a touch probe scanner10 and a discrepancy of 40 µm has been reported when a laser scanner was used.8 Our results are similar to those described in a study where conventional impression and production of stone casts, which is currently considered as the gold standard, produced a mean deviation of approximately 3 µm.12 Although there was a statistically significant difference between the mean discrepancies for the different tooth types, the maximum difference of 2.5 µm (6.3 µm-8.8 µm) is unlikely to be clinically significant.
In this study, there was greater variation in the premolar scans than in scans of the other tooth types. This may be related to the long and narrow shape of premolar impression (average axial length, 4.47 mm; buccal lingual width, 6.18 mm; and mesio-distal width, 3.60 mm) which was difficult to reach by the light beam (Fig. 4). The notion that the accuracy of the scan is impaired by accessibility of the light beam is supported by the finding of the greatest discrepancies being at the axial walls in all types of teeth.
In contrast to the digitization of models, digitizing of impressions had more difficulties in applying for practical procedure. It has been reported that mechanical tactile digitization using a probe is inaccurate, mainly owing to the easily deformable nature of the rubber impression materials during probing.10 Although one study concluded that impressions could be digitized with a high repeatability by a laser scanner, the 40 µm discrepancy reported may be inappropriately high for clinical use.8 To the best of our knowledge, our findings, which are comparable to those reported with conventional methods, are the first to support the use of a white light scanner in digitization of rubber impressions for a clinical procedure.
Laser scanners and white light scanners both have advantages and shortcomings. For example, the accuracy of white light scanners is generally regarded to be superior to that of laser scanners in which: (1) error is inevitable because of the "speckle effect", which originates from the laser beam; and (2) the laser beam is only projected on to the object once to obtain 3D coordinates from the image.13 The superior accuracy of white light scanners is mainly due to repeated rearrangement and recombination of the 3D images, which are obtained from more than 1 angle, to get a complete 3D shape data.14 White light scanners measure objects at a speed of 3 MHz/s, which is much faster than laser scanners with speeds of 10-500 kHz/s, and this may save time in the clinic.9 However, there are some limitations in the performance of white light scanners. Because of the straight linear nature of the light projection, there may be areas of shadow when scanning impressions with slender, long negative forms or acute apical angles, as seen in some anterior teeth. In this study, most discrepancies, as can be seen clearly on the color-difference maps, were observed on the vertical axial walls of the impressions of abutment teeth. Further study is needed to enhance the accessibility of the light beam to potentially shadowed areas, possibly by making more intricate movement of platform tables possible, or by increasing the numbers of cameras.
It is important to consider that the high repeatability achieved in this study may reflect the use of idealized models in an in vitro environment. In vivo studies are needed to demonstrate that a similar result can be achieved by using white light scanners in a clinical setting: Using prepared abutment teeth in the oral cavity and taking impressions in the presence of soft tissues and body fluids.
CONCLUSION
The repeatability of the digitizing abutment teeth's silicon rubber impressions by using a white light scanner was improved, compared to that with a laser scanner, showing only a low mean discrepancy between 6.3 µm and 8.9 µm, which was in an clinically acceptable range. Premolar impression with a long and narrow shape showed a significantly larger discrepancy than canine and molar impressions. Further study is needed to increase the digitizing performance of the white light scanner for deep and slender impressions.






 XML Download
XML Download