

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Every occupation has its own hazards and risks. Occupational hazard is defined as a risk to a person in his working environment. It can be a fatal accident, minor to severe injuries, allergic and systemic effects. Besides these consequences which occur immediately, there are those that appear at a latter period. According to World Health Organization the term "hazard" refers to an inherent property of an agent, or situation having the potential to cause adverse effects when an organism, system, or population is exposed to that agent.1 "Risk", by contrast, means the likelihood of causing adverse health effects. An individual's exposure to a hazard determines the degree of risk and associated untoward effects. The main objective of Occupational Safety and Health Administration (OSHA) is to promote awareness among the employees about work hazard and how to protect themselves.
Dental work set up poses many risks to its employees. A Norwegian survey, found that one half of the public health dentists reported occupational health complaints such as dermatoses (40%), eye, respiratory and systemic complaints (13%), and musculoskeletal problems (3%).2 A New Zealand study found over 40% of dental professionals affected with hand dermatoses and irritations to eyes, nose, and airway at some point in their career, and women dentists experienced double the chances of allergy occurrence.3
In prosthodontic clinics, the potential risk to irritant chemicals, inhalation of vapors, dust particles, injury from high speed rotary equipments and inflammable materials does exist. Thermal injuries from autoclaves, Bunsen burners, and furnaces can happen quite commonly. Methacrylates, rubber glove allergens, natural rubber latex proteins, and glutaraldehyde are potential allergens that lead to urticaria and occupational asthma in susceptible personnels.4
The hazards in a prosthodontic practice may be broadly classified as infectious, non-infectious, ergonomic and psychosocial (Fig. 1). The intent of this conventional review is to highlight the occupational hazards and risks associated in Prosthodontic practice and to briefly discuss their management tactics in routine practice with a view to enhance awareness and take preventive measures to reduce the risk among the professionals.
MATERIALS AND METHODS
An electronic search of English dental literature was performed through PubMed and Google Scholar to obtain all the relevant studies and reviews pertaining to occupational hazards and risks. The key words for the search include health hazards, occupational exposure, occupational hazards, risk management, curing light hazards, noise pollution, ergonomic hazards. With the information sources collated from relevant studies and reviews and organizational websites, this paper tracked and arranged the hazards and risk and their management in a contextual manner.
Physical hazards
Physical hazards that are commonly encountered in prosthodontic practice include direct physical trauma, heat and fire injuries to the face and the scalp particularly to the eye. The direct physical trauma includes accidental skin cuts and abrasions due to the usage of blunt or broken instruments or high speed projectile during trimming and polishing denture. Such trauma can act as portal entry for infections or toxic material. According to a study, percutaneous injuries occurred at a yearly rate of 3.4% among dentists. Among specialists, prosthodontists had second highest prevalence rate of 4.5%, and pedodontists, oral surgeons, orthodontists, endodontists showed 5.5%, 2.6%, 1.9%, 1.3%, respectively.5
Prosthodontic clinics and laboratory requires the use of Bunsen burners, spirit lamps and blow torches. The most common injuries in an institutional set up were burns from Bunsen burners. This was followed by injuries to the eye from needles and blades. Common causes of sharps injuries were from cleaning of probes in the sterilizing room, two-handed injection needle recapping, and burs left in handpieces.6
Grinding and polishing with vibrating tools are common in prosthodontic practice. The grinding tools are generally of high frequency and it can cause direct injury to the face and upper extremities. The effects of vibration on the hand can also result in vibration syndrome7 or vibration white finger.8 The main effects are narrowing of arteries in fingers and hands and damage to the ends of the nerves. Early symptoms include reduced blood circulation in the fingers, reduced sensitivity of the fingers to pain, touch, vibration and temperature, blanching of one or more finger tips.
Eye injuries
Traumatic injuries to the eye in prosthodontic practice are more common due to the usage of high speed rotating instruments which can generate projectiles up to 9 m/s which are often hot, sharp and infected. Symptoms include lacrimation, pain, conjunctivitis, corneal abrasion and blurring of the vision.9 More significant hazards are caused by laboratory materials. Painful reactions are elicited when methyl methacrylate monomer or pumice which contains lime and quartz are accidentally splashed into the eye; in addition pumice can also cause abrasion.10
Curing lights are commonly used for polymerization of restorative resin materials. They emit intense blue light in the range of 400 to 500 nm wavelength. According to a report, the increased ocular risk occurred at about 440 nm.11 High irradiance of blue light can be toxic to test animals, cellular structures, and human fetal retinas.12 When the blue light strikes the retina, they inhibit the formation of cytochrome-C-oxidase, which transports oxygen to photoreceptors and other retinal cells. Without cytochrome-C-oxidase, degeneration of retina occurs.13 The effects of blue light exposure could be of cumulative or acute depending on its nature. Back reflectance of blue light from teeth and other reflective surfaces leads to cumulative exposure, while acute exposure results from direct exposure to the light source. Generally, 10 - 30% of the curing light is reflected towards the operator.14 Potential ocular damage occurred after cumulative viewing of about 6 seconds at a distance of 30 cm (over an 8-hour workday) with high powered curing units.15
Noise
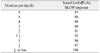
Noise levels at a given intensity and duration in any environmental situation is a potential health hazard. Loss of hearing and tinnitus are the common side effects of noise beyond the permissible levels in a set up. National Institute of Occupational Safety and Health (NIOSH), in the year 2001, included occupational hearing loss in a list of 21 priority areas for research.16 Hearing loss may be classified on the basis of exposure pattern to acoustic trauma (few exposures, intense sound level), temporary threshold shift (temporary hearing change following exposure to noise) and permanent threshold shift (result of accumulation of exposure to noise; irreversible).17 According to OSHA, exposure to 85 dB of noise, known as an exposure action value, for more than eight hours per day, can result in permanent hearing loss.18 Prosthodontists and laboratory technicians are exposed to noise of different sound levels that are potentially damaging to hearing which include lows-peed handpieces, high-speed turbine handpieces, ultrasonic instruments, high-velocity suction, and cleaners, vibrators and other mixing devices, and model trimmers.19 These equipments can emit sounds ranging from 66 dB to 91 dB (Table 1).18 In a recent study, Mojarad et al. reported that the maximum noise level in dental offices, although often beneath the damaging noise level for the human ear, was very close to the limit of hearing loss (85 dB).20
Chemical hazards
In clinical prosthodontic practice and in the laboratory, a number of synthetic and naturally occurring chemicals which include eugenol-containing materials, alloys, polymer materials, acrylic resins, ceramics, cements, sealers, etchants, hypochlorite, waxes, and elastomeric impression materials are used.21 Polymethylmethacrylate resins contain accelerators (amines), co-polymers, such as butyl-methacrylate, plasticizing agents such as di-butyl-phthalate, and inhibitor such as hydroquinone and cadmium salt-based colouring agents. These ingredients do not pose any problem for the patients but is deleterious to the technicians during packing, grinding and finishing prostheses.22 Metals, especially chromium, cobalt, nickel, beryllium and gold alloys are used for metal ceramic restorations. Dental technicians are exposed to respirable metal fumes and grinding dust during grinding and polishing of cast dental restorations. A study reported that 53 of 70 dental technicians were affected by pneumoconiosis which could be caused by dust from the processing of dental materials.23
Beryllium is added to some base metal alloys used for crowns, fixed and removable partial denture frameworks to facilitate castability by lowering the melting temperature and surface tension and to increase the porcelain metal bond strength. Exposure to beryllium vapor or particles is associated with contact dermatitis and chronic granulomatous lung disease, known as chronic beryllium disease (CBD).24 In addition, beryllium and some beryllium compounds in vapor and in particulate form have been shown to be carcinogenic based on human epidemiological and animal experimental models. Tumors linked to beryllium include lung carcinoma and osteosarcoma.25 Potential hazards or risks from exposure to beryllium result from melting, grinding, polishing and finishing procedures. The risk is greatest during the casting process in the absence of an adequate exhaust and filtration system. OSHA reported occurrence of CBD among dental laboratory technicians and, advised to implement precautions to minimize exposure to beryllium-containing dust.26
Ceramic materials are generally regarded as inert, but dust particles from these materials during handling, manipulating, adjusting and finishing the restorations represent a potential problem for the laboratory and clinical personnel. NIOSH recommend exposure limit of 0.05 mg/m3 for such dust particles. Inhalation of dust containing free silica or silicon dioxide particles in ceramic laboratories leads to silicosis.27
Irreversible hydrocolloid powder contains about 60% diatomaceous earth. When fluffed, these particles in the size of less than 3 µm in diameter and greater than 20 µm in length can be inhaled and may prove to be a health risk (carcinogenic) over a long time span.28 Woody et al. monitored and characterized aerosol particles from two alginates and showed that 10 to 15% of the particles pose the greatest risk. With daily utilization of irreversible hydrocolloid materials in the dental office, improper handling of the materials could be hazardous to the health of dental personnel.29 With regard to elastomeric impression materials, Roberta et al. tested polyethers and vinyl polysiloxanes for cytotoxicity, and the polyether materials were found to be more toxic than vinyl polysiloxanes.30
Latex gloves dusted with cornstarch powder are more often used in dental practice. Corn starch is allergenic and gives immediate allergic reactions. Starch particles combined with latex protein allergens become airborne, and is inhaled, or absorbed by our skin.31 In vitro evaluation of natural latex, synthetic rubber, and synthetic polymeric glove materials showed various degrees of cytotoxicity; this introduced silicone, powder-free gloves which has less risk.32
Biological hazards
Bacterial contamination from spatter and aerosol dissemination generated by high-speed instrumentation remains a significant risk for dental personnel.33 The main entry points of infection for a dentist include epidermis of hands, oral epithelium, nasal epithelium, epithelium of upper airways, epithelium of bronchial tubes, epithelium of alveoli, and conjunctival epithelium.34 Apart from microorganism contamination, the composition of aerosol produced during the use of rotary instruments is of concern. Research indicated that these aerosols contain silica particles from the adhesive resin fillers and various bur material byproducts. The sizes of these particles have been estimated between 2 µm and 30 µm, thus falling within the hazardous-product particle range of 2.5 µm. The concern about the small size of these particles relates to the fact that they are implicated in many diseases as they can reach the alveoli.35
Contaminated impressions (soiled with blood and other infectious material) are another source of infection in Prosthodontic practice. When plaster is poured into a contaminated impression, the microorganisms from its surface spread into the cast, and this infected cast is handled in the dental laboratory. The plaster dust from the infected casts gets into the respiratory tract, settles on clothes and environmental surfaces, and remains viable for a considerable time. For example, Mycobacterium tuberculosis remains dangerous for several weeks.36 McNeill et al. stated that impression material can act as a vehicle for the transfer of both pathogenic bacteria and viruses and cause cross contamination in the clinic and from the clinic to the laboratory.37 Another study reported cross-infection potential of impression compound and concluded that the pathogenic species of hospital bacteria like Staphylococcus aureus, Actinobacter baumanii, Capnocytophaga species, Actinobacillus species, Viridans Streptococci, and Morganella morganii were found in every step of impression making and cast pouring.38
Other possible sources of infectious contamination are dental unit waterlines (DUWL), handpieces, saliva ejectors and suctions, other devices attached to air and waterlines, and radiology equipment.39 The threat from DUWL comes from opportunistic and respiratory pathogens such as Legionella species (causative agent of Pneumonia, Legionaries' disease), Mycobacterium species, and Pseudomonas species. Higher titres of Legionella antibodies were noted for dentists with occupational exposure to Legionellae.40
Ergonomic hazards
Ergonomic hazard is a physical factor within the environment that harms the musculoskeletal system. Dental professionals are notably affected with musculoskeletal diseases in their career. The potential manifestations include various musculoskeletal disorders (MSD) that are characterized by the presence of discomfort, disability or persistent pain in the joints, muscles, tendons and other soft parts. The risk factors comprise repeated movements and prolonged awkward or forced body postures. 41 According to a prevalent study, 62% of dentists reported at least one musculoskeletal compliant, 30% showed chronic complaints, 16% had spells of absence, and 32% sought medical care.42
Prosthodontists are at high risk of neck and back problems due to the limited work area and impaired vision associated with the oral cavity. These working restrictions frequently cause them to assume stressful body positions to achieve good access and visibility inside the oral cavity which result in awkward positions over long periods of time; which in turn result in back problems. The symptoms include low back pain, stiffness, and sciatica with neurological features such as tingling, paresthesia, and muscle weakness.41 An electromyographic study by Milerad et al. and coworkers identified that shoulder, neck and arm muscle were placed under the most stress by routine dental work.43 In another study, the Nebraskan dentists reported that crown and bridge work was most likely to evoke altered sensations in their upper limbs.44
Tendinopathies and Carpal tunnel syndrome were associated with both repetitive work and forceful work. The hand performs many complex tasks, and the tendons move inside tendon sheaths with synovial fluid. Repetitive and forceful movements and the use of vibrating tools increase fluid accumulation and inflammation. Symptoms can appear from any activity causing prolonged increase in passive or active pressure in the carpal canal.45 According to Fish and Morris-Allen, 47 percent of carpal tunnel syndrome subjects in the general population were work-related and often associated with repetitive motions.44
Psychosocial hazards
Occupational stress such as coping with difficult or uncooperative patients, over workload, constant drive for technical perfection, dissatisfaction in treatment is common among dentists. Kay and Lowe reported that the most common factors contributing to stress at work were patient demands (75%), practice management/staff issues (56%), fear of complaints/litigation (54%) and non-clinical paperwork (54%).46 These physical and emotional demands result in physical and mental burnout. A comparison of stress levels and coping stress in male and female dentists showed that stress levels were similar, although women experienced more personal and domestic stress. Regarding coping response, both sexes exhibited similarity in most respects, except that women were more inclined to discuss their problems.47
Management of hazards and risks
The basic goal of OSHA is to educate employers and employees about the work place hazards, risk assessment, and risk management strategies.48 The degree of risk might depend on several factors including age, personal susceptibility, total daily exposure, exposure measured over the years, and medication. It is the responsibility of professionals and technicians to understand the specific risk factors or hazard agents and formulate an effective preventive management protocol. Table 2 outlines management strategies to reduce the risk among professionals.
Modern prosthodontic practice is equipped with sophisticated work area designs with adequate ventilation and advanced armamentarium that could possibly reduce noise pollution and risks associated with chemical and ergonomic hazards. Use of masks and aspirators, and mechanical removal of as much resin as possible before using rotary instruments may reduce the biological exposures. An orange shield used with the curing equipment adequately filters blue light between 350 nm to 500 nm. Apart from this, blue light filtering spectacle with side shields help to protect against reflectance and scatter. Decontamination of DUWL includes the state of the art method using ozone. Incorporation of ozone generating units into the dental treatment unit would be the logical extension of this technology. The integration of the use of ozone into a dental unit extends a system of disinfection and sterilization for DUWL into the clinical management and patient arena.49 Measures to combat stress by relaxation, exercise, meditation, hobbies are recommended.
CONCLUSION
Several occupational hazards and risks remain a serious concern in a prosthodontic practice, particularly MSD, contact dermatitis, high speed projectiles and bio-aerosols. Understanding the various risks will educate the professional for a better work practice and care of personal health. A mere knowledge of such hazard and familiarity with its characteristics is not sufficient for an individual to assess the potential threat. An understanding of the extent of exposure to the hazard, and strategies for minimizing the effects of occupational hazards and risks should be followed for a safe and healthy practice.


 XML Download
XML Download