

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Prolonged retention of tooth enhances the possibility that dentist may treat the patients with severe tooth wear without any invasive procedure. Tooth wear is generally considered as a result of natural physiological process. On average, the occlusal wear is estimated to be 29 µm per year for molars and 15 µm per year for premolars.1 Some endogenous or exogenous factors (e.g.; tobacco chewing) accelerate the normal wear rate and results in pathologic tooth wear. Tooth wear as a result of parafunctional habits is anticipated to progress approximately 3 times faster than physiological tooth wear.2,3 The etiologic factors include bruxism, gastroesophageal reflux disease and congenital anomalies such as Weyer's acrodental dysostosis and Dentinogenesis imperfecta.4,5 Predicting a suitable differential diagnosis is difficult in such cases due to the possibility of combination of these processes in developing occlusal wear.6
Although 'full-mouth rehabilitation' is the treatment of choice for generalized tooth wear, it is not always true applied to all clinical conditions. That is why a more comprehensive occlusal rehabilitation approach may be used to manage generalized tooth wear when the coronal tissues are moderately worn, and only some teeth require endodontic and restorative treatment. A prior endodontic restoration in worn dentition with an acceptable existing vertical dimension at occlusion and established occlusal relationships not only simplifies the treatment procedures but also makes it economically efficient. An overlay denture is partial or complete removable denture fabricated over retained roots or teeth that are not prepared with a coping to interfere with the denture.7 Overlay dentures has part of their components that covers the occlusal surface of the abutment teeth to restore them into a functional occlusion.8-10 The present article described an unique prosthodontic management of a pediatric patients suffering from rare hereditary disorders wherein the tooth development and morphology is severely impaired.
Case selection and treatment planning considerations
In the present clinical report, the overall health of patient was good with no relevant medical and dental history that could contradict the proposed dental rehabilitation. Initial intraoral assessment revealed wear of the maxillary and mandibular dentition that compromised esthetics. To establish a sound treatment strategy, a meticulous and extensive evaluation was executed, including intraoral examination of the teeth, extraoral radiography (OPG: Orthopantomogram) at access the endodontic treatment status of teeth and condition of supporting structures. The extraoral examination includes an analysis of occlusion, middle and lower facial height, vertical dimension at occlusion, esthetics and phonetics consideration. Oral hygiene status was also estimated to predict the treatment prognosis. Diagnostic casts were made and mounted in centric relation in a semi-adjustable articulator using face bow to estimate the interocclusal space and to select appropriate prosthesis. An outline of significant findings which determines the selection of future prosthesis (overlay complete denture) is presented in Table 1.
Technique
Although the fabrication of overlay complete denture is similar to that of adult complete denture, certain imperative consideration should be taken into account while fabricating a pediatric overlay denture.
Primary and final impression procedures are completed similarly as in an adult denture. In younger children, the buccal and labial vestibule are relatively superficial which needs to be recorded carefully during border molding to ensure proper fit of the custom tray to the denture foundation tissues. The selection of denture teeth may be difficult because of patient's primary or mixed dentition and must be carried out in consultation with parents and patient's esthetics.
The maxillary central incisors are arranged in such a way that it touches the vermillon border of lower lip when fricative sounds are being pronounced.11,12 The occluso-gingival length of maxillary central incisors was estimated on the basis of golden proportion.13,14 Dentures are processed, delivered and post insertion instructions are given. Follow-up period is deemed important and it includes recall appointment on regular basis for oral hygiene instructions, and minor denture adjustments. In caries-prone children, fluoride gel may be applied on the tissue surface of denture. Denture modifications can be done by adding acrylic to the area where teeth erupt or by making concavities into the dentures to accommodate the erupting teeth. In long-term denture usage (when child is grown up), it may be necessary to reline or rebase the denture or remake it due to the changes that occur in the alveolar ridge with the growth and development of the child.15
Practical considerations of overlay dentures in pediatric patients
Dawson16 suggested that in response to wear of teeth, adaptive remodeling processes occur in alveolar bone, compensating such tooth wear. Hence, it is always advised that patients with excessively worn dentitions, accurate assessment of vertical dimension at occlusion must be performed before the initiation of treatment. The use of overlay dentures to increase the vertical dimension at occlusion is very beneficial in the patients who require more comprehensive fixed prosthetic treatment in later stages.17 Keeping in mind the possibility of fixed prosthetic treatment of pediatric patients in adulthood, it is advisable to make use of such prosthesis (overlay denture) which do not alter the dentition permanently during the period of assessment and accomplish patient's functional and esthetic demands.
The complete overlay denture has several advantages when applied to pediatric patient: enhanced masticatory efficiency, esthetics, improved speech and restored vertical dimension. Preservation of alveolar bone with its use may be confirmed in the comparative analysis of lateral cephalograms of pre- and post- treatment phases. Also the retained natural teeth with their periodontal ligament offers ample of proprioception compared to a complete denture that is fabricated over an edentulous ridge.18,19 The overall management and treatment approach for generalized tooth wear in pediatric patient may be summarized as in flow chart shown in Fig. 1.
CASE REPORT
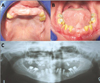
A 13-year-old male with a known history of Weyer's acrodental dysostosis reported to the dental clinic with the chief complaint of difficulty in eating and poor esthetics of the existing denture. History revealed that a denture had been fabricated 2.5 years ago, but no longer fitted. Intraoral examination showed extensive tooth wear extending to the cementoenamel junction in most areas of the teeth. Additionally, several findings related to the syndrome were noticed like partial ankyloglossia, widely spaced teeth, discolored malformed dentition, oligodontia, large pulp chambers, and collapsed bite (Figs. 2A and 2B). Radiographic finding includes multiple impacted teeth, multiple missing permanent tooth germs, retained teeth, short roots and enlarged and open pulp chambers (Fig. 2C). The fabrication of overlay denture was planned to restore the lost vertical dimension of occlusion and to improve the associated class III facial profile (Figs. 3-5). Most evidently, the patient's attitude, self-confidence and quality of life had enhanced (Fig. 6). As the available tooth structure is insufficient for future fixed prosthodontic treatment, relining/rebasing of existing denture or fabrication of new overlay denture is planned for long-term usage.
CONCLUSION
Complete overlay dentures are comparatively simple to fabricate and render satisfactory results as in present case report where the pediatric patient had an excellent treatment outcome. The major advantages include: low treatment cost, short chair time, reversibility, alterability, maintenance of alveolar bone and preserved proprioception, and excellent retention and stability. Most outstandingly, there is also a great deal of psychological benefit to the child patient.






 XML Download
XML Download