

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
PROCEDURE
Fabrication of CMPs
Enfold boxing wax (Deepti Dental Products, Ratnagiri, India) around the outside edge of the maxillary and mandibular mounting plates to form diverging housing for holding the dental plaster (Fig. 1).
Reduce the boxing wax for the maxillary and mandibular mounting plates such that the diameter at the opening is 6.5 cm.
Similarly, trim the height of maxillary boxing wax at 2.5 cm and that of mandibular boxing wax at 2 cm.
Pour a mix of dental plaster (Kalstone, Kalabhai Karson, Mumbai, India) to fill both the divergent cylinders.
Allow the dental plaster to set and remove the boxing wax (Fig. 2).
Carve a horse-shoe shaped groove on the flat surfaces of both the divergent cylinders thus formed (Fig. 3).
Form a mix of self cure acrylic resin (DP cold cure, Dental Products of India, Mumbai, India) into two spools and place over the grooves of both the maxillary and mandibular divergent cylinders to form U-shaped positive replica of edentulous ridges. Adjust the vertical height of the ridges to 5 to 6 mm.
Trim these acrylic edentulous ridges with fissure bur to make buccal and lingual undercuts that will provide port for the putty impression material during subsequent mounting of the dentures (Fig. 4).
Finish and polish both the customized mounting platforms.
Chair-side remounting of the dentures
Check the intaglio surface of each denture in the mouth with pressure-indicating pastes or waxes and make the needed adjustments.3,4
Make a centric relation inter-occlusal record with a soft medium such as warm Aluwax (Bite Registration Wax, DupleP Global, Mumbai, India) to confirm closure without contact of the denture teeth or bases.4
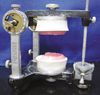
Attach the maxillary and mandibular CMPs in the articulator (Fig. 5).
Place the putty impression material (Zetaplus, Zhermack, Rovigo, Italy) in the form of a U-shaped roll over the mandibular acrylic resin edentulous ridge on the CMP and position the mandibular denture on it.
Secure the maxillary denture over mandibular denture with the help of the centric interocclusal record in aluwax, place the putty material in the denture in the region of alveolar ridge, and close the upper member of the articulator into the putty material.
After the putty impression material has set, open the articulator and remove the interocclusal record (Fig. 6).
The putty material serves as remount casts (Fig. 7).
Close the denture onto articulating paper (PD, Vevey, Switzerland) and adjust the occlusion (Fig. 8).







 XML Download
XML Download