

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Success of complex prosthodontic procedures is enhanced by accurate simulation of the condylar path of patient on an articulator. It enables the clinician to estimate the correlation between the path traced by the condyle during mandibular movements and the morphology of the occlusal surfaces which in turn aids in restoring the occlusion without interferences.1 Condylar guidance by definition (GPT-8) is the mandibular guidance generated by the condyle and articular disc traversing the contour of the glenoid fossa.2
If condylar guidance is not recorded accurately, it will lead to occlusal interferences during mandibular movements. This may also increase chairside denture adjustment time, which can be frustrating for both the patient and the dentist.3
The condylar guidance inclination in semi-adjustable articulators is set either by protrusive or lateral interocclusal registrations4-7 recorded in a suitable recording medium. Several extra oral and intra oral methods are used to clinically record condylar guidance. Extra oral methods are generally exemplified by Gysi and McCollum and mainly used in edentulous patients.8 Interocclusal protrusive wax records, Lucia jig, leaf gauge and intra oral tracers are the most commonly used intra oral methods. Several studies have shown the unreliability of recording and reproducing condylar guidance using these methods.9,10 Varying inclinations have been reported with consecutive registrations, between operators, between recording materials, and between articulators.9,10 Apart from the previously mentioned methods, condylar guidance can also be measured from radiographs. Compared to clinical methods, radiographic measurement involves stable bony landmarks and can be standardized.
Literature indicates the use of11-13 lateral cephalograms, pantomographs and tomographs for recording condylar guidance. Studies have shown that radiographic methods can record condylar guidance more accurately than other methods. The added expense, inconvenience and radiation exposure concerns are said to be the main deterrents for widespread usage of radiographic methods to estimate condylar guidance. Additionally, there is little evidence in literature to suggest it in comparison with the prevalent methods. Recently, digital CT scans have made them safer, more accurate and comparatively cheaper resulting in their widespread application in many areas of dentistry. It can be argued that application of advanced imaging is unwarranted in Prosthodontics. Yet, the higher levels of safety, accuracy and ultimate patient benefit from advanced digital imaging suggests that time may be ripe for its introduction into prosthodontics. However, evidence based adoption of digital CT scans for stomatognathic measurements and calibration of the dental articulators calls for definitive comparative studies in this area. This study, therefore, aimed at comparing condylar guidance measurements made using CT scans, interocclusal wax records, interocclusal jigs and intra-oral tracer in healthy adults.
MATERIALS AND METHODS
Before starting the study, ethical clearance was obtained from the institutional ethical board. A total of 12 patients within the age group of 20-40 years, of either sex were selected according to the inclusion and exclusion criteria. Inclusion criteria included having almost full complement of teeth, class I molar relation and 2-4 mm of overjet. Exclusion criteria included patients with temporomandibular disorders, any progressive periodontal disease, major restorations, gross attritions, poor general health, lack of adequate neuromuscular control of jaw movements and pregnancy.
1. Radiographic method
A CT scan (Somaton Sensation 40, Siemens Erlanger Germany) of mid facial region was obtained of selected subjects. Axial cross sections extending inferiorly from inferior orbital rim to approximately middle of body of ramus were obtained and reconstructed using appropriate software (Syngo fastView VX57H31, Siemens Erlanger Germany). Sagittal plane 3-D reconstruction of the region was performed on the desktop computer. The Frankfort Horizontal Plane (FHP) and a line along the posterior slope of articular eminence (AE) was drawn, extending from the superior anterior most point on the glenoid fossa to the most convex point on the apex of articular eminence (AE).
The angle between FHP and posterior slope of AE was measured to obtain condylar inclination angle. This was done for both right and left sides of the subject to obtain right and left condylar inclination angles (Fig. 1).
2. Clinical methods
Maxillary and mandibular casts were mounted on semiadjustible articulators (Protar 7, KaVo Dental GmbH, Bismarckring, Biberach) with the aid of facebow and centric relation record.
1) Interocclusal wax record method
The patient was trained to move the mandible forward till the teeth were in edge to edge relationship. A two-sheet thick wax rim was adapted to the maxillary arch. Patient was then asked to do the movement as practiced before. This wax record was reinforced with zinc oxide eugenol bite registration paste (Bosworth Superbite) for accurate details (Fig. 2).
2) Lucia jig
Impression compound was used to fabricate the Lucia jig. Patient was trained to move the mandible forward till the anterior teeth were in edge to edge relationship and close without perforating the jig. Subsequently silicone bite registration material (Regisil Rigid, Superfast Set) was injected between the occluding surfaces of the teeth (Fig. 3).
3) Intra-oral tracer
An intra oral tracer was attached to the acrylic plate and the Gothic arch tracing was obtained. Protrusive record in silicone bite registration material was recorded at 6 mm of protrusion. This record was used to adjust the articulator and thereafter the condylar inclination angles were measured (Fig. 4).
RESULTS
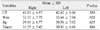
Mean CG left and right angle measurement values obtained from the CT scan method were 42.42 and 43.83 degrees, respectively while it was 33.64 and 33.33, 30.56 and 29.16, 30.83 and 31.25 degrees for interocclusal protrusive wax record, Lucia jig, and intraoral tracer methods, respectively. Statistical analysis showed insignificant difference between the right and left side mean HCG values (Table 1, Fig. 5).
The mean values obtained from the wax, jig and intra oral tracer methods provided low Pearson correlation values for the right (R = 0.423 wax, R = 0.354 jig, R = 0.265 tracer) as well as the left side (R = 0.237 wax, R = 0.494 jig, R = 0.125 tracer) when compared with the CT values. This indicates very little or no association between the values obtained by those methods and CT values.
Comparison of mean HCG values obtained from different clinical methods showed that tracer method has medium level of association with wax and jig methods which was statistically insignificant. However, jig and wax methods showed strong level of association which was statistically significant (Table 2, Fig. 6).
DISCUSSION
The left and right condylar guidance angles of each subjects was measured using the four methods. The difference between the left and right measurements obtained from different methods was statistically insignificant. However, there is some evidence in the literature contrary to the results obtained in this study. el-Gheriani and Winstanley14 and Zamacona et al.1 have reported significant variation between the left and right condylar guidance values. The difference with Zamacona's results can be attributed to the heterogeneity of the sample - a mix of partially edentulous and completely edentulous subjects where as in the present study; the sample was more homogenous, consisting of only partially edentulous subjects. It must also be noted that the study employed only the graphic method. The disagreement with results from el-Gheriani and Winstanley, on the other hand, may be due to the fact that all the subjects in their study was those who were referred for treatment for TMJ disorders vis-a-vis healthy young adults employed in the present study.
The HCG values obtained from CT scan were greater than those obtained from clinical methods. Also the results obtained indicate that the clinical methods exhibit low levels of association with CT scans. Brewka15 in 1981 stated that radiographic methods and clinical methods are in disagreement. Christensen and Slabbert12 in a 1978 review has stated that "no radiographically determined sagittal condylar guidance angle coincided with that obtained with the use of intra-oral records. The radiographically determined angle showed a greater mean value than that determined by intra-oral records". Among the clinical methods, values obtained from the jig method exhibited medium level of association with those obtained from the tracer and strong level of association with those obtained from wax method. This difference may be attributed to the 6 mm protrusion in the tracer method while edge to edge position was used in wax and jig methods. One important reason for the inconsistency of intra oral methods may be that, regardless of the material used, sagittal condylar angle changes with the degree of protrusion,16 and that intra-oral record represents only one point along the condylar path.17
Various methods used to record condylar guidance angle clinically have been often reported to exhibit wide variations between each other. Graphic methods offer values different from those of wax interposition based on Christensen phenomenon.18 There is relative inconsistency and lack of precision in the currently available clinical methods for measuring condylar guidance angle. Results from previous studies9,10 have also reported significant differences between instruments and methods and also between consecutive registrations for the same patients. Gross et al.9,10 have reported that Whip Mix consistently gave the highest angulations and Hanau the lowest, in the same patients. The present study supports previous studies showing intra oral methods of recording condylar guidance angle have lower levels of reproducibility and are subject to variations of instrument, operator, and occlusal records.9,19
In general, it could be inferred from the present study that none of the clinical methods were found to be giving condylar guidance angle values comparable with the CT while the clinical methods among each other shows moderate to high amount of association. Given the increased precision and chemo-mechanical properties of modern day techniques and materials it is only natural to suggest that computerized tomographical methods of measuring condylar determinants must be introduced into the clinical work flow. However, clinical methods are more practical, economical and are consistent with each other. Hence, it is not advisable, on the basis of these results to nullify their utility.
Finally, the results of this study need to be viewed by keeping in mind it's certain characteristics and features. Semiadjustable articulators were used in the study for receiving the records from the clinical methods. They are limited in their capabilities to accurately simulate the TMJs, the jaws and their movements because of the fixed inter condylar distances and the straight condylar pathways, which are reported to cause errors especially in the horizontal and frontal plane18 and arbitrary hinge axis is being used to transfer the facebow record to the articulator. This might be the reason for variance between the CT and rest of the methods. It must be noted that CT scans are superior in precision and standardization than all the other methods. The type of CT scan used for the study may not be available for bulk of dentists, especially those who are practicing in rural and semi urban areas. Future studies should investigate the possible effect that TMJ disorders might have on clinical methods. Inspite of these factors, this study represents an important step forward in the direction of improving accuracy of condylar guidance angle determination in prosthodontic rehabilitation. It may be beneficial to employ CT scans for condylar measurements especially for complex oral rehabilitations. However, further studies with larger sample sizes are required to confirm the results of the present study.
CONCLUSION
It can be concluded from the present study that (1) the right and left HCG values were comparable to each other to a limited degree, (2) CT scans gave higher mean HCG values than those obtained from the clinical methods, (3) HCG values obtained from all the clinical methods were comparable with each other.







 XML Download
XML Download